Sub-Arachnoid Hemorrhage (SAH)
Introduction
A subarachnoid cerebral hemorrhage (SAH) is a bleeding in the brain where blood leaks into the space between the brain and the meninges (the protective layers surrounding the brain).
The space is called the subarachnoid space. It is approximately one centimeter thick and is located between the pia mater and the arachnoid membrane. Within this space are vital blood vessels that supply and drain the brain. An SAH therefore occurs in the area where important blood vessels meet.
A SAH is often accompanied by a very sudden, severe headache that comes on out of nowhere. The intensity of this headache is often the worst headache anyone has ever experienced.
It is sometimes described as a "thunderbolt" headache. Patients often experience nausea with or without vomiting. The headache may radiate to the neck and shoulders.
However, 12%-51% of patients with an SAH are initially misdiagnosed. Their headaches were diagnosed as migraines or tension headaches.
Symptoms
- Sudden onset
- Maximum pain (97% of cases) within seconds or minutes of onset
- Often severe ("worst headache of life")
- Usually nausea or vomiting
- In rare cases, there is no headache, but for example only neck pain or sudden confusion.
An SAH is a relatively uncommon brain hemorrhage. Approximately 3-5% of all strokes are SAHs. About half of SAH cases occur in people under 55. Therefore, a relatively young group of people is often affected.
Every brain hemorrhage has a huge impact, but when a family with young children and work life are also turned upside down, the consequences are even more severe.
What makes an SAH particularly concerning is that a vulnerable period begins in the two weeks following the SAH. In some cases, new symptoms occur as a result of a new stroke.
In order to closely monitor these and other potential consequences, people with an SAH have to stay in the hospital for approximately two weeks.
Causes
Brain Aneurysm
The cause of a SAH is often the rupture of a brain aneurysm.
An aneurysm is a dilation of the blood vessels (sometimes a balloon-like shape) that, over time, develops into a weakness in the blood vessel. In some people, aneurysms develop in the brain in a major blood vessel network at the base of the brain. This network, the Circle of Willis, acts like a roundabout for blood flow.
There is a high chance that such an aneurysm will rupture when there is a sudden large increase in blood pressure, for example, due to physical activity, but an aneurysm can also rupture "out of the blue." Whether you develop an aneurysm is often a matter of bad luck. Smoking, alcohol, and drug use are risk factors for developing an aneurysm. Genetics also play a role. Women have a higher risk of developing an aneurysm than men.
Perimesencephalic Hemorrhage
Perimesencephalic hemorrhage literally means: bleeding around the midbrain (mesencephalon). The mesencephalon is a part of the brainstem. The blood from the hemorrhage accumulates in the midbrain cisterns.
Cisterns are extensions of the subarachnoid space through which cerebrospinal fluid circulates. A perimesencephalic hemorrhage is a subarachnoid hemorrhage that is not caused by an aneurysm. Approximately 10%-15% of SAH bleeds are perimesencephalic hemorrhages.
Physical impairment is often minimal or completely absent. Loss of consciousness or decreased level of consciousness is rare.
Complications, such as hydrocephalus, reduced cerebral ischemia, and new hemorrhages, are rare.
The prognosis is generally better than a SAH after an aneurysm, in terms of survival rate and clinical course (how quickly someone can recover during hospitalization).
However, the invisible consequences of this type of brain injury are often underestimated. There are often many consequences, such as fatigue, disrupted stimulus processing, or cognitive impairment.
According to researchers, a third of people with a perimecencephalic hemorrhage still experience symptoms after five years. See, for example, this study and the study linked here. It is therefore recommended that this group of patients also receive long-term follow-up after discharge from the hospital.
No known cause
In some patients, no underlying cause is found. This is called an angiographically negative SAH. Sometimes the blood is mainly visible around the brainstem (perimesencephalic SAH), in which case it is suspected to originate from a small venous or capillary blood vessel.
In other cases, the bleeding pattern is more diffuse, but still without demonstrable vascular abnormality. Possible explanations include a small vein hemorrhage, a clotting disorder, vasculitis, a dissection (tear in the blood vessel wall), a rare connective tissue disease, or a dural fistula.
A dural arteriovenous fistula (DAVF) is a direct connection between an artery and a vein in the dura mater. This causes increased pressure in the vein that carries the blood.
A tangle of blood vessels, also called an arteriovenous malformation (AVM), may be another, but rare, cause. An AVM, like an aneurysm, is a weak spot in the vascular system which may cause bleeding.
The breakdown of the causes of SAH in figures
Where in the brain? Meninges
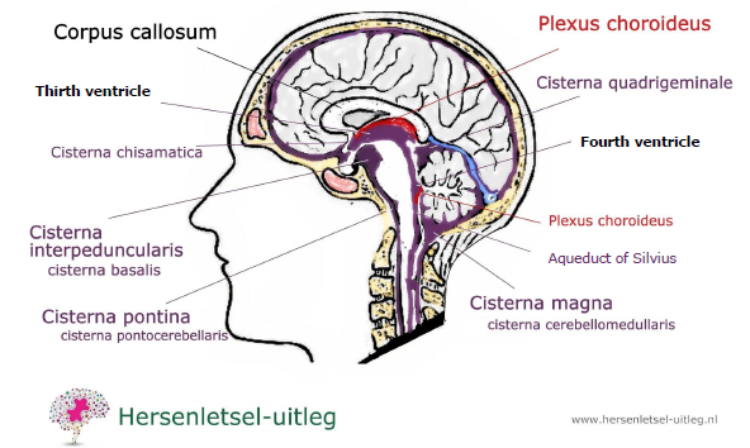
In the drawing below, you see the subarachnoid space in purple, with the ventricles (or cerebral cavities) and scattered cisterns, through which the cerebrospinal fluid flows.
The meninges surround the brain. These meninges nourish the brain and also serve as a cushion, protecting it.
The layers are constructed from the outside in:
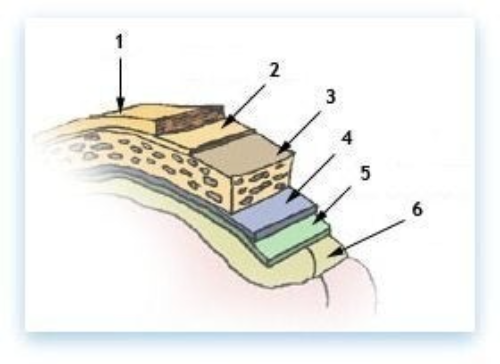
The meninges are located around the brain. The meninges perform a function in the supply to the brain and also serve as a pad for the protection of the brain. The layers around the brain are (from outside to inside):
• Scalp (1)
• Periosteum (2)
• Bone (3)
• Dural (Dura Mater (4))
• Arachnoid (5)
• Subarachnoid space (this is where the SAH occurs)
• Soft meningeal (Pia mater (6))
Pressure on the brain
When an aneurysm grows and ruptures, a SAH (subarachnoid hemorrhage) occurs between the brain and the skull.
The skull is hard and doesn't allow the bleeding to drain, which increases pressure on the brain.
The released blood causes increased pressure/swelling in this area of the brain. The brain cells in that area then receive insufficient oxygen and nutrients, and may die.
Shortly after a subarachnoid hemorrhage, there may be a disruption in the drainage of cerebrospinal fluid (CSF). In that case, the ventricles of the brain are filled with blood instead of CSF. This is also called an intraventricular hematoma (IVH). This may also cause increased intracranial pressure.
The optic nerves are vulnerable to increased intracranial pressure.
The greatest threat of an intraventricular hematoma is the development of acute hydrocephalus with occlusion. If this leads to neurological deterioration, it must be treated urgently with a drain (external ventricular drainage / EVD) via an intraventricular catheter (IVC). A ventricular drain is also called a shunt.
Because a subarachnoid hemorrhage is a cerebral hemorrhage, we refer you to the cerebral hemorrhage page for more information.
Diagnosis & Treatment
After experiencing an SAH (or suspecting an SAH), you should call 911 as soon as possible and go to the hospital. The first goal is to determine whether it was indeed an SAH and, if so, what the underlying cause was. This is done with a CT scan. If the CT scan shows that an aneurysm has ruptured, surgery is required to reduce the risk of further bleeding.
Coiling
Two methods are used. The first method (called coiling) involves guiding small coils through a vein in the groin to the site of the aneurysm. The aneurysm is then filled to prevent further bleeding.
Clipping
The second method involves brain surgery in which the aneurysm is surgically closed from the outside. This method is called clipping.
Long-term treatment depends entirely on the severity of the hemorrhage and whether or not you experienced complications or disability.
Sometimes there's a period when professional help is needed. Sometimes you can recover at home without professional assistance. On our consequences page, you can read about visible and invisible consequences, which can potentially occur with any type of brain injury, including SAH.
Long-term expectations
A recent study conducted at the University Medical Center Groningen (Khosdelazad et al., 2023) demonstrated that there were few to no differences in changes in cognitive functioning between the subacute phase (3-6 months after SAH) and the chronic phase (2-4 years after SAH) in patients who had an SAH due to an aneurysm (aneurysmal/aSAH) compared to patients who did not have an aneurysm (non-aneurysmal SAH/anSAH).
An aneurysm is a localized dilation or bulge in an artery. This vulnerable spot in the cerebral artery can rupture and cause a cerebral hemorrhage.
A large number of patients continued to experience cognitive impairment and reduced well-being up to four years after the hemorrhage.
Moreover, no differences were found between aSAH and anSAH patients in terms of cognitive impairment, cognitive complaints, and symptoms of anxiety and depression.
Based on this study, it is therefore recommended in clinical practice to offer both groups of SAH patients the same aftercare program, with a neuropsychological assessment in the subacute phase (approximately six months after the SAH), which also focuses on well-being.
This way, patients can become aware of the potential limitations they may experience after the SAH and, if necessary, can receive personalized treatment.
More information:
https://my.clevelandclinic.org/health/diseases/17871-subarachnoid-hemorrhage-sah
https://en.wikipedia.org/wiki/Subarachnoid_hemorrhage
https://www.nhs.uk/conditions/subarachnoid-haemorrhage/
https://www.mayoclinic.org/diseases-conditions/subarachnoid-hemorrhage/symptoms-causes/syc-20361009
https://www.hopkinsmedicine.org/health/conditions-and-diseases/subarachnoid-hemorrhage
Resources
Boereboom, W., Jacobs,E., Khajej,L., van Kooten, F. Ribbers, G.M. Differences in cognitive and emotional outcomes between patients withperimesencephalic and aneurysmal subarachnoid haemorrhage. https://doi.org/10.2340/16501977-1236
Eyskens, E., Feenstra, L., Meinders, A. E., & Vandenbroucke, J. P. (1997). codex medicus (10de editie). Maarssen, Nederland: ElsevierGezondheidszorg.
Hartwijzer. (z.d.). Consulted 5th of december 2015, from https://www.hartwijzer.nl/
Hersenletsel-uitleg: https://www.hersenletsel-uitleg.nl/soorten-hersenletsel-hersenaandoeningen/beroerte-cva/hersenbloeding/sub-arachnoiedale-bloeding-sab-1
Hersenstichting. (z.d.). Hersenstichting - Home. Consulted 5th december 2015, van https://www.hersenstichting.nl/?gclid=EAIaIQobChMIh8L_h_OI3wIV0uJ3Ch3T6gvLEAAYASAAEgJHu_D_BwE
Homepage van Heliomare. (z.d.). Consulted 5th december 2015, van https://www.heliomare.nl/Khosdelazad, S et al 2023 Investigating Recovery After Subarachnoid Hemorrhage With the Imaging, Cognition andOutcome of Neuropsychological Functioning After Subarachnoid Hemorrhage (ICONS) study
https://pure.rug.nl/ws/portalfiles/portal/250291669/PDF.pdf
Kuks, J. B. M., Snoek, J. W., Oosterhuis, H. J. G. H., & Fock, J. M. (2003). Klinische neurologie (15de editie). Houten: Bohn Stafleu Van Loghum.
Lindbohm, J. V., Kaprio, J., Jousilahti, P., Salomaa, V., & Korja, M. (2016). Sex, Smoking, and Risk for Subarachnoid Hemorrhage. Stroke, 47(8),1975–1981. https://doi.org/10.1161/STROKEAHA.116.012957Macdonald RL, Schweizer TA. Spontaneous subarachnoid haemorrhage. Lancet. 2017;389(10069):655–666.
doi: 10.1016/S0140-6736(16)30668-7. [DOI] [PubMed] [Google Scholar]
NVN - Nederlandse Vereniging voor Neurologie :: Home. (z.d.). Consulted on 5th of december 2015, from https://www.neurologie.nl/
NVvN – Nederlandse Vereniging voor Neurochirurgie. (z.d.). Consulted 5th december 2015, van http://www.nvvn.org/
Oplossingen voor een sterk hart | Hartstichting. (z.d.). Consulted 5th december 2015, van https://www.hartstichting.nl/
Rasyid A, Mesiano T, Kurniawan M, Hidayat R, Mulyadi R, Nugroho SW, Yolanda S, Wiyarta E, Harris S. Spontaneous subarachnoid hemorrhage dueto arteriovenous malformation mimicking migraine: A case report. Radiol Case Rep. 2021 Dec 31;17(3):790-793. doi:10.1016/j.radcr.2021.12.015. PMID: 35024077; PMCID: PMC8732334.Rinkel GJ, Wijdicks EF, Vermeulen M, Ramos LM, Tanghe HL, Hasan D, et al.. Nonaneurysmal perimesencephalic subarachnoid hemorrhage: CT andMR patterns that differ from aneurysmal rupture. Am J Neuroradiol 1991; 12: 829–834. https://pubmed.ncbi.nlm.nih.gov/1950905/
De Vries EA, Boerboom W, Van den Berg-Emons RJG, Van Kooten F, Visser-Meily JMA, Ribbers GM, Heijenbrok-Kal MH. Fatigue is Associated withReduced Participation and Health-Related Quality of Life Five Years After Perimesencephalic Subarachnoid Haemorrhage: A Multicentre Cross-Sectional Study. J Rehabil Med. 2022 May 11;54:jrm00271. doi: 10.2340/jrm.v54.212. PMID: 35191989; PMCID: PMC9131194.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9131194/