Ventricles
Introduction
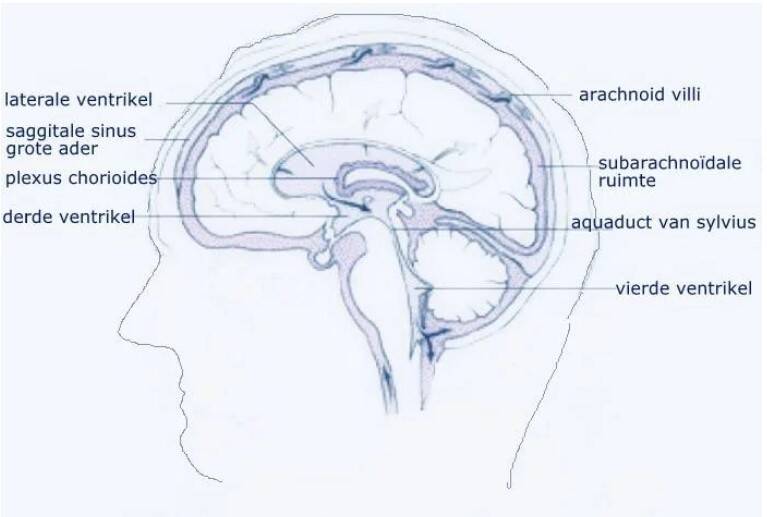
Deep within the brain there is a system of four irregularly shaped cavities called the cerebral chambers, ventricles or cerebral cavities. Each cerebral hemisphere has a lateral ventricle.



Fourth ventricle in red
Thirth ventricle in red
Lateral ventricles in red
Corridors of cavities and canals
The brain chambers are connected to each other through channels and openings. These cavities produce and contain a clear, watery fluid called cerebrospinal fluid or CSF.
In terms of composition, the fluid resembles blood plasma, but it contains more hydrogen ions (H+).
Other names for this fluid:
- Cerebrospinal fluid
- Liquor
- Spinal fluid (the fluid below the brainstem)
This cerebrospinal fluid circulates and this flow ultimately ends up in the spaces around the brain, meninges and spinal cord where it is absorbed into the bloodstream at the surface of the brain at the subarachnoid space.
Cerebrospinal fluid production
In the ventricles (both side ventricles, third and fourth ventricles) there is a network of capillaries called the choroid plexus.
Here, 400 to 500 milliliters of cerebrospinal fluid is produced every day by specialized brain cells.
This fluid is replaced several times a day. This is necessary because the brain can only contain a total of 150 milliliters of cerebrospinal fluid. So there is a permanent production, transport and breakdown of cerebrospinal fluid and there is a natural balance between production and drainage. If this balance is disturbed, the pressure may be increased or decreased.
Function of cerebrospinal fluid
The cerebrospinal fluid serves as a cushion for the brain and spinal cord. The brain floats, as it were, in this fluid and the fluid absorbs the first blows in the event of a collision. The fluid also nourishes the nerve cells and removes waste products from the nerve cells and helps regulate the temperature.
Development
In the development and growth of the brain ventricles, as with other parts of the nervous system, three phases can be distinguished.
- The embryonic phase (from fertilization to the eighth week),
- The fetal phase (from the ninth week to birth),
- The neonatal phase (first four weeks after birth).
Increased cerebral pressure due to too much cerebrospinal fluid
The consequence of illness or damage may be that cerebrospinal fluid production increases, disrupting the balance of supply, transport and breakdown.
When the cerebrospinal fluid cannot drain properly or is not or is barely absorbed into the bloodstream, the brain ventricles will become enlarged.
This is called ventriculomegaly.
This increase in cerebrospinal fluid results in increased cerebral pressure. The optic nerves are vulnerable to increased cerebral pressure. The increase in moisture creates a situation of hydrocephalus (hydro=water, cephalus=brain). Read more on our page on hydrocephalus.
Diseases and damage
There may be several causes for the increase in the production of cerebrospinal fluid or the disruption of the transport between the cavities or the drainage of the cerebrospinal fluid.
- Disruption in the drainage of cerebrospinal fluid due to a
meningitis, - Disturbance in the drainage of the cerebrospinal fluid shortly after a sub-arachnoid hemorrhage (SAH). In that case the ventricles are filled with blood,
- Intraventricular hemorrhage or intraventricular hematoma (IVH), the occurance of a bleeding in the ventricles,
- 1st degree; the hemorrhage occurs in a small area of the tricles,
- 2nd degree; the bleeding also occurs in the ventricles,
- 3rd degree; the ventricles expand and become larger due to the blood,
- 4th degree; there are also hemorrhages in the brain tissues surrounding the ventricles.
Such an intraventricular hemorrhage is often a cerebral hemorrhage in the first days of life of a baby who was born prematurely, often with a low birth weight.
Intraventricular hemorrhage (IVH) in adults usually occurs with aneurysmal subarachnoid hemorrhage (SAH) or a cerebral hemorrhage caused by high blood pressure (hypertension-related intracerebral hemorrhage).
The greatest threat of IVH is the development of acute hydrocephalus/hydrocephalus with occlusion. If this result in neurological deterioration it must be treated urgently with a drain (external ventricular drainage /EVD) via an intraventricular catheter (IVC). A ventricular drain is also called a shunt.
- Adhesion after a cerebral hemorrhage, after infections, an accident, or after tumors (benign and malignant),
- Congenital defect,
- Constriction of the connection between the third and fourth ventricle,
- Disturbance in the development of the fourth ventricle
- Brain tumor
- Tumor in the production organ of cerebrospinal fluid (plexus papilloma)
- Enlarged brain chambers/enlarged ventricles after traumatic brain injury/post traumatic ventriculomegaly. This is reported on average in one third of patients after traumatic head injury,
- Normal Pressure Hydrocephalus due to old age, even resembles a dementia picture. Also called NPH; Normal Pressure Hydrocephalus. See the hydrocephalus page.
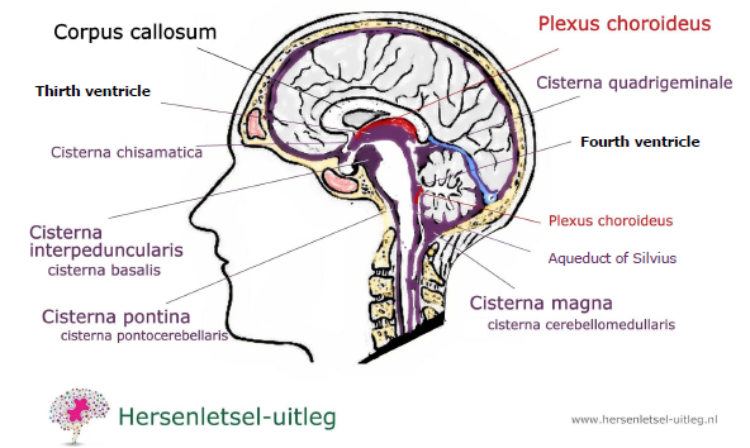
Cisterns
Difference between cisterns and cerebral ventricles:
- The ventricles produce and distribute cerebrospinal fluid within the brain, as described above.
- The cisterns serve as storage sites for cerebrospinal fluid and play an important role in its flow. In addition, some cisterns also provide space for blood vessels and nerves. Because these cisterns are interconnected, it is important that they remain open to allow the cerebrospinal fluid to flow freely.
Where in the brain?
These widening spaces, also called subarachnoid cisterns, are located within the subarachnoid space and outside the brain.
Here, the pia mater and the arachnoid mater are slightly further apart. This is because the arachnoid mater runs over the folds and grooves of the brain, while the pia mater precisely follows the shapes and contours of the brain.
A subarachnoid hemorrhage is possibly one of the main causes of swollen cisterns. In this condition, one or more cisterns become filled with blood, which can increase pressure within the skull. This can lead to serious symptoms and complications.
Conditions affecting the cisterns
Increased intracranial pressure may compress the cisterns.
A skull fracture may cause damage leading to cerebrospinal fluid leakage, blood pooling (such as a subarachnoid hemorrhage), or pressure on these areas. This can cause increased pressure in the brain, which can be life-threatening.
An arachnoid cyst is a fluid-filled cavity between the layers of the arachnoid membrane. These cysts are usually present from birth and arise from a problem in the early development of the nervous system. In many cases, arachnoid cysts cause no symptoms and are discovered incidentally during scans, such as an MRI or CT scan. If symptoms do occur, they may include headaches, a feeling of pressure, dizziness, or nervous system problems.
Infections such as meningitis may also cause swelling and irritation.
In addition, tumors or cysts near the cisterns can disrupt the normal flow of cerebrospinal fluid, which also leads to complications.
If someone experiences severe headaches, nausea, changes in consciousness or difficulty moving, or neurological deficits, contact a doctor immediately.
Some Important Cisterns
The specific spaces in the subarachnoid space of the brain where cerebrospinal fluid (CSF) circulates are named after their location.
- The cisterna magna, also called the posterior cerebellomedullary cisterna, is a space at the back of the brain. It lies between
the cerebellum and the medulla oblongata. It is one of the largest spaces in the brain.
- The interpeduncular cisterna, also called the basal cisterna, is located at the base of the brain between two brain structures (the cerebellar peduncles). It is surrounded by important parts such as the hypothalamus.
The cisterna magna and interpeduncular cisterna are also called basal cisterns.
- The pontine cisterna, or pontocerebellar cisterna, lies next to the brainstem, between the pons and the cerebellum. It helps these parts of the brain work together. The basilar artery runs through the pontine cisterna.
- The chiasmatic cisterna is located around the optic chiasm, the area where the optic nerves (nervi optici) cross at the base of the brain.
- The quadrigeminal cisterna, or superior cisterna (cisterna venae magnae cerebri), is located at the back of the midbrain (the mesencephalon), around the colliculi (tetrahedral plate), and is important because of its proximity to nerve pathways for seeing and hearing (visual and auditory structures).
- The ambiens cisterna surrounds the midbrain (the mesencephalon) and extends along the lateral edge of the brainstem. This cisterna plays an important role as a passageway for nerves and blood vessels, including the external optic nerve (fourth cranial nerve or nervus trochlearis) and the posterior cerebral artery (arteria cerebri posterior/ACP).
There are more cisterns, but they are of less clinical significance. See:
https://radiopaedia.org/articles/subarachnoid-cisterns
Synonyms
The following names are also used for the cavities described above:
- Cerebral subarachnoid cavity
- Subarachnoid space
- Spatium subarachnoidale cerebrale
- Cavum subarachnoidale cerebrale
- Spatium leptomeningeum cerebrale
Spontaneous Intracranial Hypotension
Spontaneous intracranial hypotension (SIH) is a rare condition in which the pressure of cerebrospinal fluid (CSF) within the skull suddenly becomes too low.
This can occur due to a leak in the meninges, often without an obvious cause. The most common symptom is a severe headache, which usually worsens when sitting or standing upright and subsides when lying down.
Other symptoms may include neck pain, nausea, dizziness, hearing problems, and blurred vision. Treatment varies per patient but may include bed rest, drinking plenty of fluids, caffeine, or, in more severe cases, a so-called "blood patch," in which the patient's own blood is injected to seal the leak.
Spontaneous Intracranial Hypotension
Spontaneous intracranial hypotension (SIH) is a rare condition in which the pressure of cerebrospinal fluid (CSF) within the skull suddenly becomes too low.
This can occur due to a leak in the meninges, often without an obvious cause. The most common symptom is a severe headache, which usually worsens when sitting or standing upright and subsides when lying down.
Other symptoms may include neck pain, nausea, dizziness, hearing problems, and blurred vision. Treatment varies per patient but may include bed rest, drinking plenty of fluids, caffeine, or, in more severe cases, a so-called "blood patch," in which the patient's own blood is injected to seal the leak.
Idiopathic intracranial hypertension (IH / IIIH)
In idiopathic intracranial hypertension (IH/IIH) there is increased cerebral pressure. There is a high cerebrospinal fluid or
CSF pressure caused by a disturbance in the balance between production and drainage of cerebrospinal fluid. Idiopathic means that there is no explanation for the congestion of the cerebrospinal fluid. Intracranial means it is within the skull.
Sometimes it is caused by medication, sometimes in excessive vitamin A use, in diseases such as Besnier Boeck, Lupus Erythematosus.
It is also possible that it is caused by other blood diseases, in which thrombosis may occur, an accumulation of inflammatory cells in the draining cavities (venous sinuses) or other causes of the chronic clogging of these cavities.
It may also be that too much cerebrospinal fluid is produced.
Obesity, especially in women between the ages of 20 and 44, has been associated with this condition. Possibly also through use of the contraceptive pill, which can increase the tendency of the blood to clot. This can cause the cavities to silt up. This rarely happens, see this study.
The complaints may be similar to those that occur with a tumor in the head: headache, nausea, vomiting, blurred or less sharp vision, loss of visual field and double vision.
Characteristic is a narrowing of the field of view at the outer edge. With increased pressure in the head, the place where the optic nerve enters the eye (the entry point) has blurred edges (pupillary constriction). There is fluid accumulation (edema) in the optic nerve head. This is called papilledema or optic nerve swelling. The optic nerve may be permanently damaged by the increased pressure (papillary atrophy).
In practice it is difficult to distinguish between headaches from migraine and from idiopathic intracranial hypertension (IHH).
If there is no headache and no papilledema, the diagnosis of IIH cannot be made. Sometimes an MRI scan
necessary to be able to find the abnormalities if no papilledema was initially found.
Other complaints may include: pain in the neck, back, shoulders or arms, throbbing ringing in the ears (pulsating tinnitus), photosensitivity, nausea, cognitive complaints.
Synonyms for IIH
Sometimes the following outdated terms are still used to refer to Idiopathic Intracranial Hypertension:
- Benign Intracranial Hypertension (BIH) = benign high pressure in the brain
- Pseudotumor cerebri (PTC) = a pseudo brain tumor
It sometimes happens that the ventricles of the brain merge, which makes it difficult to install a drain to remove excess cerebrospinal fluid.
Increased brain pressure may also be due to the brain swelling after an accident. This is dangerous because the brain cells become compressed. The neurologist will make every effort to lower the pressure in the brain.
The patient is put asleep and pain relief is given. Medicines to lower the pressure are administered and a pressure monitor can be inserted through a thin tube by the neurosurgeon.
Research shows that patients with IIH have an increased risk of obstructive sleep apnea syndrome (OSAS).
Post-traumatic ventriculomegaly
After traumatic brain injury, on average, a third of patients develop a variant of hydrocephalus; post-traumatic ventriculomegaly, literally translated: enlarged ventricles.
This enlargement of the brain chambers was seen in 39.3% of cases after severe head injury. There was then no connection with age.
After moderate traumatic brain injury, it occurred in 27.3% of patients. It was clearly visible on a scan at 4 weeks post-injury in 57.6% of those affected and at two months in 69.7%. This problem is often overlooked.
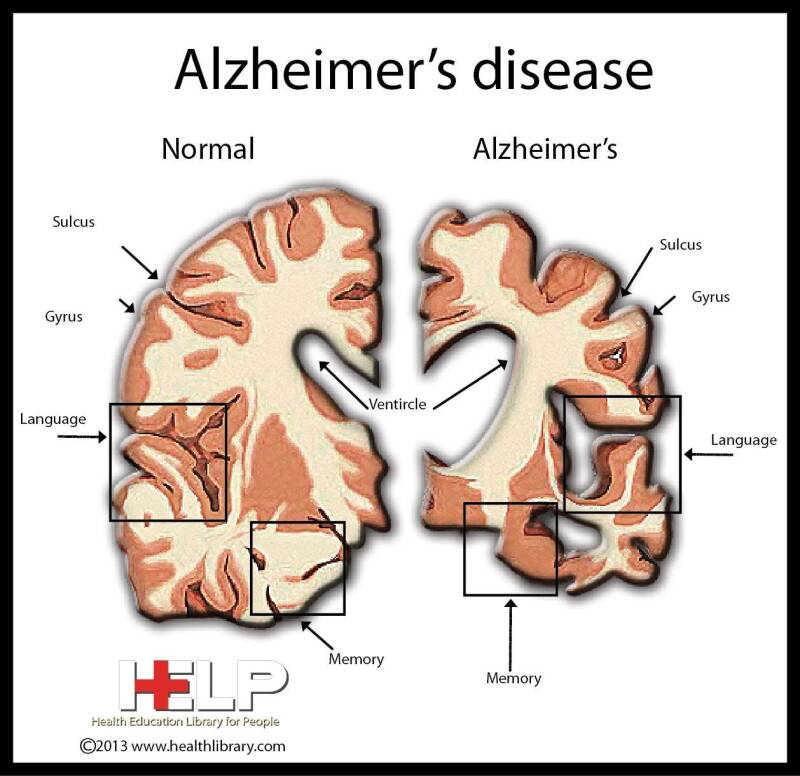
Enlarged Alzheimer's Enlarged ventricles (ventriculomegaly) in Alzheimer's
Enlarged brain ventricles generally indicate brain atrophy = shrinkage of the brain, but this is also seen with normal aging.
In Alzheimer's disease, enlargement of the brain chambers also occurs because the brain tissue decreases. The cerebral cortex is shrinking.
Resources
Drake, R.L., Vogl, W. and Mitchell, A.W.M. (2005), Gray’s Anatomy for Students, Elsevier Churchill Livingstone, London.
Edwards, R.J., Dombrowski, S.M. et al. (2004), “Chronic hydrocephalus in adults”, Brain Pathol, vol. 14, no. 3, July, pp. 325-336
Etminan, M, F. Khosrow‐Khavar, M. Sodhi, B. Carleton, L. A. Magee, H. Tremlett
Pseudotumor cerebri syndrome with different types of hormonal contraceptives in women of child‐bearing age, 18 August 2020, https://doi.org/10.1111/ene.14480
Hersenletsel-uitleg.nl
Marieb, E.N. (1998), Human Anatomy & Physiology, 4th ed, Benjamin/Cummings Publishing Company, California.
Kinsman SL, Johnston MV. Hydrocephalus. In: Kliegman RM, Behrman RE, Jenson HB, Stanton BF, eds. Nelson Textbook of Pediatrics
Rosenberg GA. Brain edema and disorders of cerebrospinal fluid circulation. In: Daroff RB, Fenichel GM, Jankovic J, Mazziotta JC, eds. Bradley's Neurology in Clinical Practice
Pictures from anatomografie (maintained by Life Science Databases (LSDB))
Naff., . Intraventricular Hemorrhage in Adults. Curr Treat Options Neurol . 1999 Jul;1(3):173-178. doi: 10.1007/s11940-999-0001-0. https://pubmed.ncbi.nlm.nih.gov/11096707/
Poca María A , Juan Sahuquillo, María Mataró, Bessy Benejam, Fuat Arikan, Marcelino Báguena (2005) Journal of Neurotrauma. 2005 Nov;22(11):1303-10 Ventricular enlargement after moderate or severe head injury: a frequent and neglected problem
Yiangou, A., Mitchell, J.L., Nicholls, M. et al. Obstructive sleep apnoea in women with idiopathic intracranial hypertension: a sub-study of the idiopathic intracranial hypertension weight randomised controlled trial (IIH: WT). J Neurol 269, 1945–1956 (2022).
https://doi.org/10.1007/s00415-021-10700-9 lateral ventricle.
Images are from Anatomography, maintained by Life Science Databases(LSDB).