Apraxia and dyspraxia
Brain injury may make it difficult for people to perform everyday tasks purposefully, even though she or he still is able to understand instructions.
Dyspraxia from birth is a motor developmental disorder. This is called Developmental Coordination Disorder (DCD). Information about this can be found here.


This disorder concerns intentional motor behavior.
It concerns actions that could be performed in a normal way before the brain injury.
The disorder does not stem from paralysis or poor coordination. It is also not caused by neglect, facial loss, and certainly not by unwillingness.
It is possible that one day something works better than another. The functioning of someone with a brain injury can fluctuate due to various factors.
This inability is called apraxia. It can make it impossible to perform all sorts of common, everyday activities, such as self-care.
Roughly speaking: not knowing how or not knowing what
There may be a disorder in planning and sequencing (ideatory apraxia), but there may also be a disorder in handling objects (ideomotor apraxia).
The person either doesn't know what to do because she or he lacks an idea or action plan, or she or he knows what to do, but does not know how to do it because the application of the correct motor program is disrupted.
Difficulty imitating movements
In some cases a person can imitate a complex action immediately after seeing it, but is unable to perform it later. Imitation may therefore be intact while commands or spontaneous actions cannot be carried out.


Different forms of apraxia
There are two main types of apraxia:
- Ideational apraxia
- Ideomotor apraxia
Learn more about different types of apraxia in the drop-down menus below.
Where is the injury located?
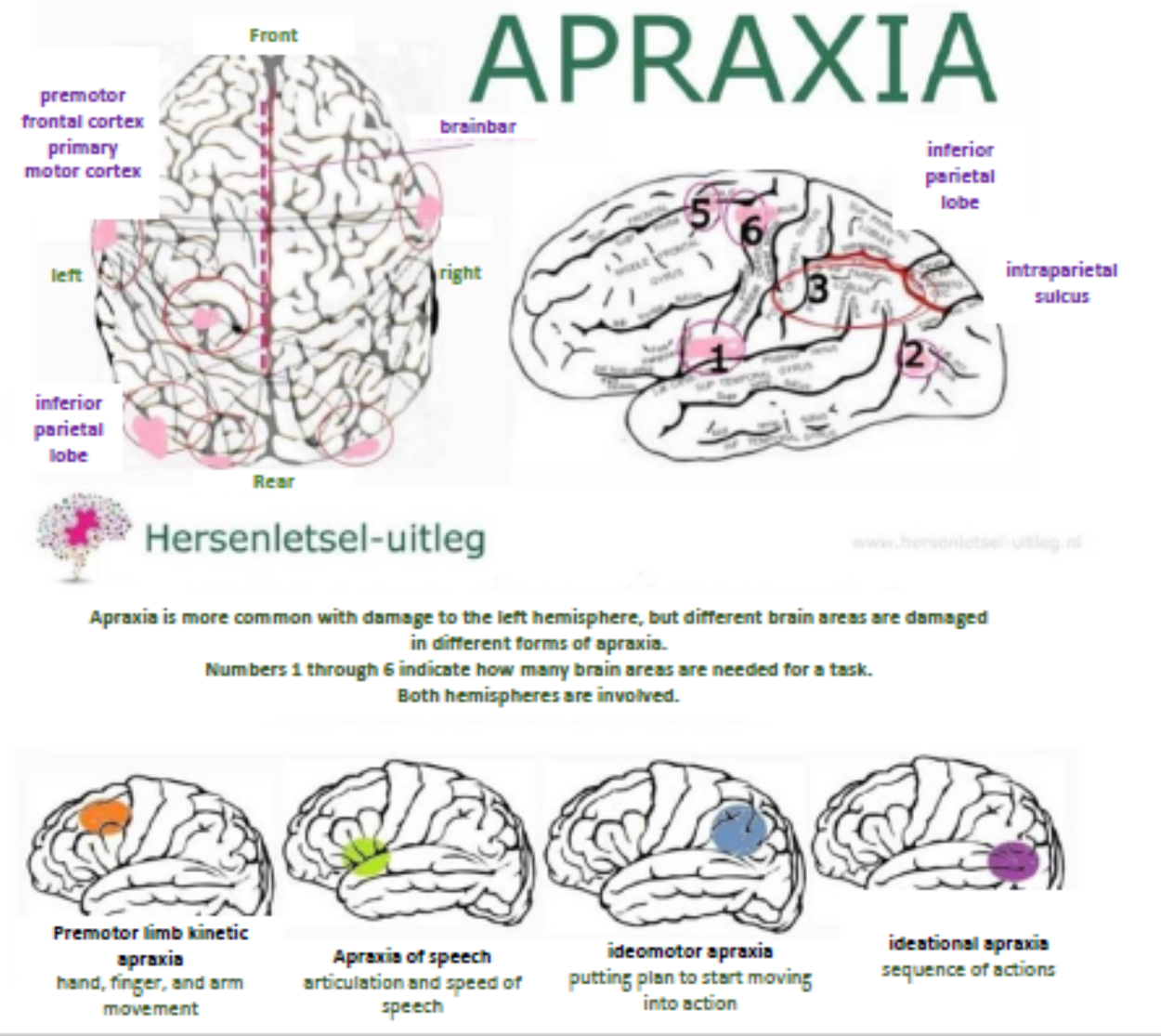
Apraxia is a motor disorder caused by damage to the brain, the posterior parietal cortex, or the corpus callosum.
The frontal lobes are important for voluntary movement, expressive language, and managing higher-level executive functions.
Lesions to the premotor frontal cortex of both hemispheres, the left (lower and posterior) inferior parietal lobe, and the brainbar (corpus callosum) may cause apraxia. Apraxia is more common with damage to the left hemisphere than to the right hemisphere and often coexists with aphasia.
- Ideomotor apraxia usually results from lesions in the left hemisphere, both frontal lesions (in the forehead) and posterior parietal lesions (in the posterior parietal lobe).
- Bilateral lesions in the left hemisphere may also result in ideomotor apraxia.
- Unilateral ideomotor apraxia on the left may result from lesions in the corpus callosum or the right premotor area.
- Lesions in the prefrontal and premotor cortex and the left inferior parietal lobe may result in ideational apraxia.
Apraxia after brain injury and forms of dementia
Apraxia may occur due to brain damage caused by acquired brain injury or various forms of dementia. A common apraxia in people with dementia is ideational and ideomotor apraxia.
In Alzheimer's disease, different forms of apraxia may occur at all stages of the disease: ideational, ideomotor, constructional apraxia (in an early stage) and buccofacial gait apraxia (in a late stage).
Frontotemporal dementia exhibited buccofacial and gait apraxia late in the disease.
Cortical-basal degeneration exhibited limb kinetic apraxia.
Lewy body dementia exhibited more agnosia and less apraxia. Agnosia is the inability to recognize things (images, sounds, smells) perceived through the senses (eyes, ears, nose, mouth, touch).
Apraxia with aphasia
Apraxia often co-occurs with aphasia. Those who only have aphasia are able to lead a relatively normal life, but in case significant apraxia is also present, the person is almost always dependent.
Tips when a loved one has difficulty performing a task
-
It may help the person with apraxia to break down the task into smaller steps or to simplify the tasks.
-
It may be helpful to provide concrete instructions while performing a task. A person may benefit from having everything prepared in the correct order or using pictograms as a step-by-step plan. A clear structure for (difficult) tasks is important. For example, by thinking about them in advance and dividing the task into steps.
-
It is important to be patient and understanding and to give the person time. It is also important to connect with the established (life) habits of the person with apraxia.
-
Establish a fixed pattern or rhythm when organizing the day and week. A daily activity schedule can help structure the day. This also reduces the number of choices to make.
-
Assign the person to tasks he or she can still perform.
Support methods and examples
Asking to perform an activity:
When your partner/loved one is sitting at the sink to wash, ask if they would like to wash their upper body. This helps them get started.
Asking questions about the activity:
If your partner/loved one doesn't show any signs of wanting to begin, ask: "What do you need?"
Clarifying the question through gestures:
Making a washing motion.
Starting the activity together:
Turn on the faucet together by taking your partner/loved one's hand and guiding it to the faucet.
Showing pictures of the activity:
If you are making coffee together, first look at the pictures of making coffee.
Preparing the necessary items, if necessary in the correct order:
Prepare the coffee, the filter, or coffee cups from specific coffee makers.
Pointing out the items:
When dressing, you can point out the items of clothing.
State what needs to be done next:
When putting on a blouse, say: take the blouse, unbutton the buttons, put your arm in the sleeve, etc.
Let each other know how the activity went:
Discuss both the steps that went well and those that caused problems.
More information
Information on apraxia can be found on the following websites:
https://medlineplus.gov/ency/article/007472.htm
https://www.ncbi.nlm.nih.gov/books/NBK585110/
https://www.asha.org/public/speech/disorders/apraxia-of-speech-in-adults
Resources
Hugo Liepman Heilman en Rothi, model van apraxie, ergotherapie richtlijn voor diagnostiek en behandeling van apraxie bij CVA-clienten,neuropsychologische behandeling.nl, hersenstichting nederland, slotervaartziekenhuis behandeling na een beroerte, btsg bibliotheek innovatie inouderenzorg, St Lievensziekenhuis neurologie, Zorgtraject OVL, Logopedie.nl, Apraxie.org, Slingeland ziekenhuis ergotherape, M.T. Banich (2004).Cognitive Neuroscience and Neuropsychology. 2e editie. Houghton Mifflin Cie en J.B.M. Kuks, J.W. Snoek, H.J.G.H. Oosterhuis. Klinische Neurologie15e druk, Bohn Stafleu Van Loghum, Houten, 2003, ISBN 90-313-4028-6 National Aphasia Association, NIH/National Institute of NeurologicalDisorders and Stroke, Adams, Principles of neurology Nadeau, Stephen E. (2007).
Gait Apraxia: Further Clues to Localization.https://doi.org/10.1159/000104714
https://www.ntvg.nl/artikelen/loopstoornissen-door-neurologische-aandoeningen
Chandra, S. R., Issac, T. G., Abbas, M.M. (2015). Apraxias in Neurodegenerative Dementias. Indian Journal of Psychological Medicine, Jan.-March,37(1): 42-47.
Retrieved from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4341309/.
Accessed on August 22, 2016 https://medlineplus.gov/ency/article/007472.htm
Hersenletsel-uitleg.nl https://www.hersenletsel-uitleg.nl/gevolgen/lichamelijke-gevolgen/apraxie-1