Thalamus

The thalamus, the yellow section on the drawing above, is an important brain nucleus and is considered one of the intermediate brain, together with the pituitary gland and the hypothalamus. It is the most 'wired' portion of the brain.
Introduction
Foreword: The brain works together as a single unit. Brain functions are distributed throughout the brain regions and arise from the exchange between the regions. Nevertheless, symptoms can be identified per brain region.
Do you only want the short summary? Then follow this link.
Do you only want to read the possible symptoms per core group and per adjacent brain regions? Follow this link.
Do you want to know more about the anatomy, functions, and potential damage per core group? Then follow this link.
Thalamus: most wired part of the brain
The thalamus is an important relay station deep within the brain. Virtually all sensory information – such as what you see, feel, and hear – is transmitted via the thalamus to the cerebral cortex.
It helps to focus attention on important information and filter out less important stimuli.
It also assists with movement, memory, emotions, and with being conscious, awake, and alert.
It plays a role in akinetic mutism. This is a syndrome, a consequence of brain injury, in which the person speaks little or not at all (mutism) and moves little or not at all (akinesia). The person may follow you with their eyes but otherwise appears apathetic and does almost nothing of their own accord.
Thalamus is derived from the Greek word for hidden central inner chamber or bedroom; θάλαμος, because it lies deep within the brain and forms the 'central' chamber.
It is a deep-seated central nucleus in the brain
- virtually all sensory information (except smell) enters it first
- it distributes and organizes information before it goes to the cerebral cortex
- it is in contact with almost all parts of the cortex via thousands of connections
You can therefore view the thalamus as the central inner chamber where information first enters and is forwarded
Senses
l
Thalamus
(central inner chamber)
l
Cerebral Cortex
Gateway to the Cerebral Cortex
The connections from the thalamus to the cerebral cortex return from the cortex to the thalamus.
This is called the thalamo-cortico-thalamic circuit. As a result, minor thalamic lesions can mimic cerebral cortex syndromes, and in some syndromes, the specialization of the cerebral hemisphere can be recognized.
As a gateway to the cerebral cortex, the thalamus has to transmit many sensory stimuli (except smell), but it must also filter stimuli, allowing healthy individuals to "shut off" certain stimuli. It is therefore one of the so-called "filters" (stimulus filters), a control center to help the brain focus on important and unimportant stimuli.
The main core groups of the thalamus and adjacent structures (in the diencephalon)
Important to know:
The thalamus works closely with other brain regions. The symptoms a person experiences may correspond to damage to a specific core group, but are often also determined by the cooperation between different brain networks.
The following anatomical terms explain the names of the core groups:
The image below is a schematic anatomical representation. The exact shape, size, and mutual boundaries of the core groups may vary slightly depending on the anatomical cross-section and the anatomical reference work.
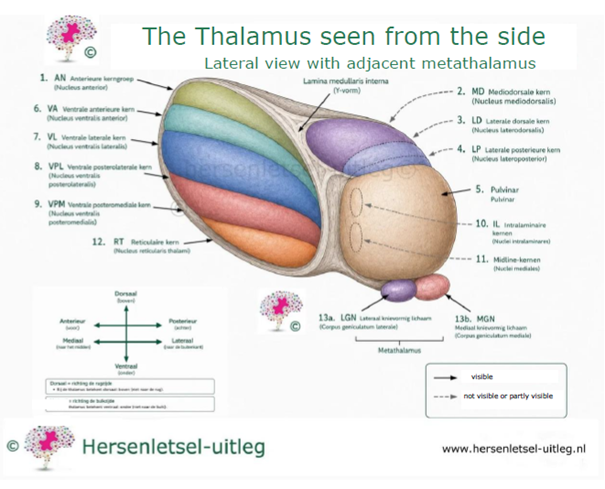
Discussion of the image of the thalamus viewed from the side (lateral view) with the adjacent metathalamus
The image shows the main nuclear groups of the thalamus in a lateral view. The thalamus consists of various nuclear groups that receive, process, and transmit information to the cerebral cortex. Not all nuclear groups are fully visible from this view. Therefore, hidden or partially hidden structures are indicated with a curved gray arrow, while straight black arrows point to structures that are directly visible.
The lamina medullaris interna (Y-shaped white matter tract) divides the thalamus into different anatomical nuclear groups.
The intralaminar nuclei are located within this white matter tract. The midline nuclei lie directly along the third ventricle and are barely visible from a lateral view. The reticular nucleus forms a thin layer on the outside of the thalamus and plays an important role in regulating the information processed by the thalamus.
Located at the posterior side are the lateral knee-form body (LGN (Medial Geniculate Nucleus)) and the medial knee-form body (MGN (Medial Geniculate Nucleus)). Together, they form the metathalamus. The LGN processes visual information, while the MGN is involved in processing auditory information.
The illustration is based on the anatomical classification as described in Gray's Anatomy, supplemented and verified with Mai & Paxinos and Blumenfeld.
For each section, we elaborate on the following:
- Where are the nuclei located?
- From where do they receive information?
- Where do they send information?
- What do these nuclei do?
- Possible consequences of damage
- What do you notice about this in daily life?
- Important to know
- In-depth information for healthcare professionals
- Anatomical references
The list is written in plain language (B1 level), but is based on authoritative anatomical and neurological literature, including Gray's Anatomy, Mai & Paxinos, and Blumenfeld. Where scientific insights are still developing, this is indicated in the text. In this way, we combine understandable explanations with current medical knowledge.
Two nuclei: the pulvinar at the back of the thalamus and a nucleus in the middle at the bottom, the nucleus reticularis thalami, have partially overlapping functions:
| FUNCTION | PULVINAR | NUCLEUS RETICULARIS THALAMI |
|---|---|---|
| Attention regulation | mostly visual | general and modeling |
| Visual processing | strongly involved | supports visual attention |
| Integration of sensory information | multisensory | filters unwanted information |
| Role in consciousness | less direct, more in perception | crucial for alertness and focus |

Here you can download a document by Emmanuel Carrera M.D. and Julien Bogousslavsky, M.D., containing more information about thalamus injury and behavior.
advertisements are not ours