Congenital brain injury

Congenital Brain Injury / Congenital Brain Defects
When people talk about brain injury, they're usually referring to acquired brain injury (ABI) that a person sustained at some point in their life due to illness or an accident. This represents a break in the lifeline.
If a brain injury occurs around birth, during or shortly after birth, or in the first year of life, it's called congenital brain injury.
There's no break in the lifeline, as there's no memory of the brain injury before it. However, congenital brain injury also has significant consequences.
quote:
Marleen, 26, says: "What I find difficult is that it always seems to be about acquired brain injury...
My congenital brain injury has had an impact on me my whole life, but you don't talk about that every day...
Acquired brain injury is also a brain injury. Look at the consequences...
I see them all in myself and in my peers."
From the seventh month of pregnancy, the brain's surface area grows significantly due to the development of the sulci and convolutions. If a baby is born before this period, the brain may not yet be fully developed, which can have consequences for the rest of its life.
When an unborn or newborn baby sustains damage, it often occurs in conjunction with a serious or stressful situation. This stress can also affect the child's brain.
The difference between congenital and acquired brain injury after birth is often difficult to determine. Brain damage is considered acquired brain injury (ABI) if it occurs six months to a year after birth.
To avoid confusion, it is often preferable to refer to the age at which the brain damage occurred, so that the consequences for development can be better assessed.
Risk of Cerebral Palsy (CP) before birth
There is an increased risk of the baby developing Cerebral Palsy (CP) due to:
- Congenital abnormalities
- Infection in the uterus (intrauterine infection). Infections with these pathogens can alter the placental environment, such as the function of enzymes and proteins. This may contribute to problems that cause birth defects.
- Cytomegalovirus, CMV (herpesvirus)
- Chickenpox
- Rubella
- Cytomegalovirus, CMV (herpesvirus)
- Urinary tract infection in pregnant women
- High fever in pregnant women
- Toxoplasmosis (infection)
- Sickle cell disorders reduce blood flow to the baby's brain
- Fetal membrane infection (chorioamnionitis), often due to prolonged labor
- High fetal bilirubin levels
- Abnormal brain development due to infections or genetic changes
- Multiple birth pregnancy
- Placental abnormalities
- Premature birth
- Cerebral infarction or cerebral hemorrhage before birth
- Fetal anemia due to, for example, folic acid deficiency
- Fertility treatments increase risk due to low birth weight
- Genetic abnormalities
- Drug or medication use by pregnant women
The following definition of CP can be found on page 9 of this document:
Cerebral palsy (CP) describes a group of permanent dis-orders of the development of movement and posture,causing activity limitation, that are attributed to non-progressive disturbances that occurred in the develop-ing fetal or infant brain. The motor disorders of cerebralpalsy are often accompanied by disturbances of sensa-tion, perception, cognition, communication, and behav-iour, by epilepsy, and by secondary musculoskeletalproblems.
See also our page on CP.
Other diseases before birth
- Rhesus antagonism
A Rhesus-negative pregnant woman is expecting a Rhesus-positive baby from a father with Rhesus-positive blood. The mother's blood containing Rhesus antibodies may break down the baby's red blood cells, causing anemia in the womb. These broken blood cells release bilirubin, which may damage the baby's brain. If an increase in bilirubin levels is detected early (through amniocentesis), intervention can be performed with an Rh immunoglobulin injection or a blood transfusion of the baby via the umbilical cord before birth. Such a blood transfusion is repeated every two weeks, and labor is induced around the 33rd week of pregnancy.
- Blood vessel abnormalities, for example, a malformation (AVM), an aneurysm, weakened blood vessels that can lead to a cerebral hemorrhage before the baby is born.
- Anemia in the baby due to a lack of folic acid in the pregnant woman. This may lead to, among other things:
- cerebral palsy in the baby (see also paragraph above)
- oxygen deficiency in the baby's brain.
-
High blood pressure in pregnant women (preeclampsia, eclampsia, HELLP syndrome) may cause insufficient blood flow to the baby's brain. Read about the consequences for the brain on the special page. High blood pressure in pregnant women may also occur as a side effect of medication.
-
Meningoencephalitis (inflammation of the brain and meninges) caused by rubella in pregnant women.
-
Benign tumors that arise in embryonic cells may be present before birth. See the page on primary brain tumors.
-
Metabolic disorders A hereditary condition in which substances in the body's cells are processed less efficiently. This can cause a specific substance or waste product to accumulate and lead to symptoms. Sometimes enzymes that regulate metabolism are missing, and sometimes the enzymes are malfunctioning. See our page on various metabolic disorders (such as Batten disease, Tay-Sachs disease, MLD, Leigh disease, and Cerebral ALD adrenoleukodystrophy).
-
Microcephaly Small skull size that prevents brain development, due to rubella in the pregnant woman, a genetic abnormality (WDR62 gene and other genes), premature ossification of the skull (craniosynostosis), metabolic disorders, or certain infections during pregnancy.
- Fetal Alcohol Syndrome (FASD), when a pregnant woman drinks alcohol, she risks brain damage to her baby.
The alcohol travels from the pregnant woman's bloodstream through the placenta into the unborn baby's bloodstream. The unborn baby's brain is still developing, and the toxic alcohol poses a direct threat. We have a dedicated page on this topic; see Fetal Alcohol Syndrome.
- Dandy-Walker syndrome is a congenital abnormality of the cerebellum and the fluid cavities surrounding it, and has several variants. Classic Dandy-Walker syndrome is characterized by:
- a non-developed or reduced-sized cerebellum
- fluid accumulation near the cerebellum
- an enlarged fourth ventricle
- the absence of the transition from the brain to the bone marrow (vermis or vermis cerebelli), which lies in the center of the cerebellum. This vermis is responsible for controlling movement
- enlargement of the posterior fossa (posterior fossa). The posterior fossa is the green area in the image below:
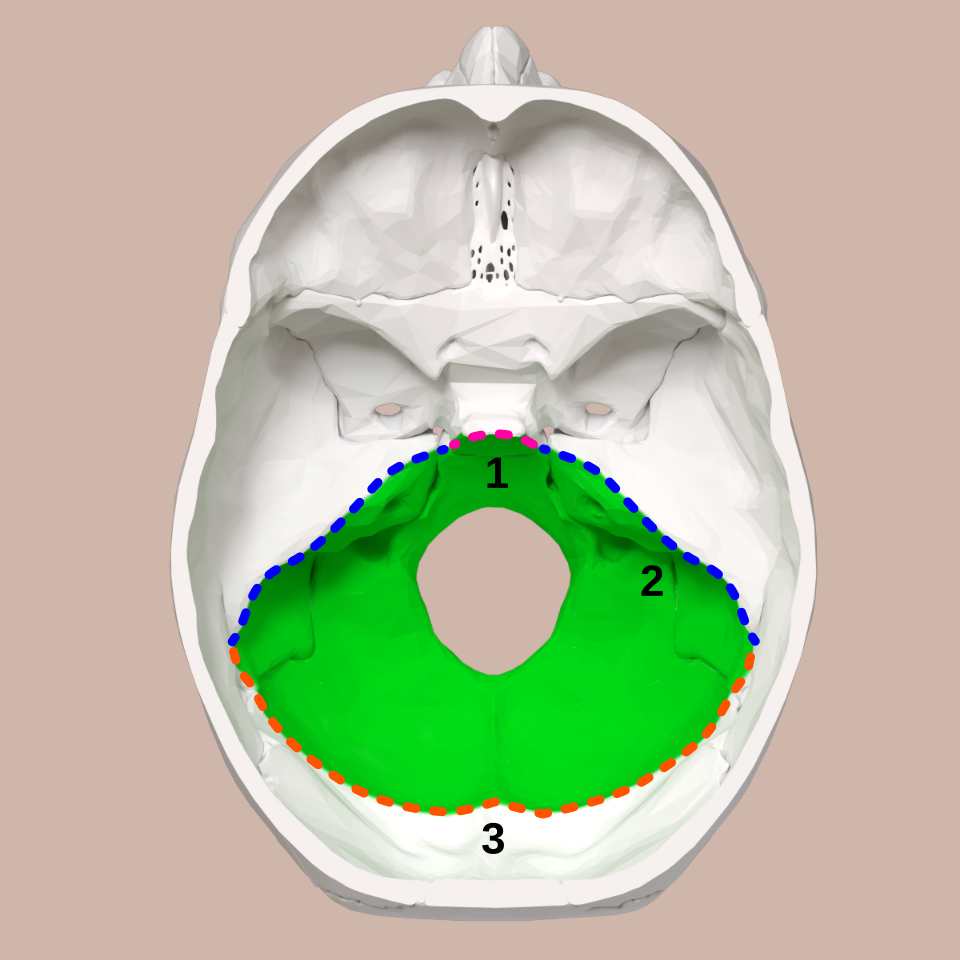
image source https://commons.wikimedia.org/w/index.php?curid=80601084
The posterior cranial fossa is the cavity in the skull where the brainstem and cerebellum are located.
It is the most posterior part of the brain and rests on the base of the skull.
The tentorium, a kind of partition, separates the posterior cranial fossa from the middle cranial fossa.
If any of the above five characteristics are present it is a case of Dandy Walker variant.
The lifespan is normal.
Causes may include rubella during pregnancy and alcohol consumption in the pregnant woman, but a genetic abnormality (ZIC1 gene, ZIC4 gene, FOXC1 gene) may also underlie this syndrome.
Characteristics A small number of children with Dandy-Walker syndrome have six toes or six or more fingers (polydactyly), or the toes or fingers are fused together (syndactyly).
Other characteristics may include breathing problems, hydrocephalus, jerky eye movements, and developmental delay. One-sixth of children with this syndrome experience epileptic seizures.
Development Cerebellar abnormalities cause widespread regulatory problems: both motor developmental problems and emotional regulation problems occur.
Children with Dandy-Walker syndrome develop more slowly than their peers and usually walk and talk later. Developing coordination is more difficult, or due to low muscle tone, children with this syndrome fall more often than others.
Some children have difficulty interacting with others. They have difficulty making contact and don't always understand what's expected of them.
In adults, there's little structured research. However, it is known that neuropsychiatric symptoms, particularly mood disorders, occur more frequently than in other people.
- Holoprosencephaly: The front of the brain is poorly developed or absent. There is no or insufficient separation between the left and right cerebral hemispheres. This results in deformities in the midface and skull. An eye, nose, or nostril may be missing. A cleft lip can occur, and there are other manifestations.
- Lissencephaly with all subtypes: a smooth brain without sulci, folds (gyria), or convolutions.
- Corpus callosum agenesis: the corpus callosum is not formed.
- Cortical dysplasia: the structure of the cerebral cortex is different from normal.
- Polymicrogyria is a genetic disorder in which the brain is constructed differently, with more small convolutions/small gyri (microgyri) in the cerebral cortex than normal. This leads to an abnormally thick cortex. This abnormality can affect one or more brain regions. The lifelong consequences can be diverse and vary in severity, such as epilepsy, difficulty with physical movement (motor dysfunction), particularly spasticity, and loss of function of the facial and throat muscles (pseudobulbar palsy/paresis). The person has difficulty chewing, swallowing, and speaking. The tongue cannot be moved properly.
- Septo-optic dysplasia (Morsier syndrome) is a developmental delay of the optic nerves of the pituitary gland and the membrane between the anterior chambers of the brain (septum pellucidum).
- Chiari malformation (an outdated term: Arnold Chiari malformation) in which the lower portion of the cerebellum no longer lies within the skull but protrudes through the foramen magnum into the spinal canal. The lowest portion of the cerebellum, and sometimes also the brainstem, is compressed. This embryonic developmental disorder is often accompanied by syrinx (a cavity in the spinal cord) or malformations of the cranial bones and vertebrae. Sometimes a Chiari malformation occurs as a result of an arteriovenous malformation (AVM).
More information: https://mayfieldclinic.com/pe-chiari.htm
-
Neural Tube Defects (NTDs) During pregnancy, early in the embryonic stage, the child's spinal column or skullcap does not close properly.
The structure is not properly formed. This may lead to:
-
Spina bifida.
Children with spina bifida usually have a physical and sometimes an intellectual disability.
-
The (near) absence of the cerebrum (anencephaly), or an open skull. Children with an open skull almost always die at or shortly after birth.
Neural tube defects (NTDs) can be prevented by approximately 60% by taking folic acid from four weeks prior to pregnancy up to and including the 10th week after the last menstrual period.
Causes of NBD include diabetes in the expectant mother that was already present before pregnancy, an extremely limited diet, the use of certain medications or chromosomal abnormalities. The 13th chromosome then appears three times instead of twice.
-
More information can be found on this wikipedia page.
During birth
- Pressure on the baby's head during birth may lead to:
- Cephalohematoma, bleeding under the periosteum and the skull.
- Subgaleal hemorrhage,a bleeding between the tendon of the frontal muscles and the periosteum. Most children with a subgaleal hemorrhage develop normally. Some develop epilepsy or blindness. Some also suffer brain damage.
- Subdural hemorrhage, bleeding under the dura mater
- Subarachnoid hemorrhage, bleeding under the arachnoid mater
- Epidural hemorrhage, bleeding between the dura mater and the skull
- Increased intracranial pressure due to bleeding pressing on the brain.
- Cephalohematoma, bleeding under the periosteum and the skull.
- During birth, the baby may experience severe shortness of breath, either due to mucus in the airways, placental rupture, umbilical cord problems, or other causes. This may lead to:
- Reduced blood flow to the brain and thus to oxygen deficiency
- Reduced blood flow and thus to oxygen deficiency to all tissues: ischemia
- Both forms of oxygen deficiency during birth may lead to cerebral palsy, although this is a small percentage. There are other factors before birth and in the first year of life that may lead to cerebral palsy.
- Not all oxygen deficiencies lead to serious damage in the baby.
- Both forms of oxygen deficiency during birth may lead to cerebral palsy, although this is a small percentage. There are other factors before birth and in the first year of life that may lead to cerebral palsy.
- Reduced blood flow to the brain and thus to oxygen deficiency
- Birth canal infections (infections in the vagina or cervix) with:
- bacteria (meningococci), which can cause meningitis in the baby
- streptococci B, which can lead to meningitis
- infection of the fetal membranes (chorioamnionitis), which can lead to cerebral palsy
- bacteria (meningococci), which can cause meningitis in the baby
- If the baby is handled too roughly (accidentally or otherwise) or falls, there is a risk of:
- traumatic brain injury with skull fracture
- traumatic brain injury without skull injury
This can also be caused by a very difficult birth in which the baby's head is pressed against the mother's pelvis for too long.
- traumatic brain injury with skull fracture
After birth
- In newborns, fetal blood is broken down, which can cause them to have a slightly yellowish appearance due to high bilirubin levels in the blood. This is normal and can last for 3 to 4 days. Bilirubin levels can be measured with a heel prick.
Above a certain limit, too much of this blood breakdown product, bilirubin, can cause brain damage. This does not always happen, but the risk is there. This can lead to attention problems later in life, or neurological symptoms or developmental disorders.
In severe cases, this can lead to:- kernicterus (due to jaundice), damage to certain brain nuclei, which can cause:
- damage to the auditory nerve (hearing loss);
- the coordination of automatic movements can be impaired (choreathetosis)
- the control of the optic nerves can be damaged (eye deviation, squinting or strabismus)
- intellectual disability can occur
- damage to the auditory nerve (hearing loss);
- kernicterus (due to jaundice), damage to certain brain nuclei, which can cause:
- Streptococcus B infection can lead to meningitis.
- Infection in the baby can lead to cerebral palsy after birth
- Shaken baby syndrome
- Blood vessel abnormalities, such as a malformation AVM, aneurysm, weakened blood vessels that can lead to a brain hemorrhage.
- If the baby is handled too roughly (accidentally or otherwise) or falls, there is a risk of:
- a skull fracture with a traumatic brain injury
- a traumatic brain injury without a skull injury
- a skull fracture with a traumatic brain injury
- Low birth weight and premature birth can sometimes lead to cerebral palsy (CP).
- Poor blood flow to the brain can lead to cerebral palsy.
- Hydrocephalus usually occurs as a result of a brain hemorrhage in the first few days of life in premature babies.
Child Development and Long-Term Consequences
Child development may be disrupted. We discuss this on the page Children with Brain Injury.
The brain's maturation for developing higher-order cognitive functions, language, and behavioral functions begins in children aged 4 to 5. These impairments may first become apparent in a child at age 5 or 6 and be noticed by you or others.
Congenital brain injury can have a wide range of physical, mental, and cognitive consequences, depending on the severity and location of the injury. Every child is unique. No injury and no child can be compared. We aim to clearly identify the causes, but the consequences vary from child to child.
Possible long-term consequences:
- Behavioral and emotional problems:
- Easily irritated
- Depressed
- Impulsive
- Suffering from emotional (mood) swings
- Lack of initiative
- Decreased self-confidence
- Cognitive problems:
- Attention and concentration problems
- Learning, perceiving, understanding, thinking
- Dyscalulia
- Language and speech problems
- Problem-solving skills
- Memory problems
- Slowed rate of information processing
- Delayed skill acquisition
- Disrupted development / a developmental break as expected
- Intellectual disability, varying in severity may occur. (See the cognition page for a complete list)
- Possible physical complaints:
- Headache
- Chronic pain
- Oversensitivity to light/sound, overstimulation
- Dizziness, balance problems
- Difficulty with coordination and balance
- Decreased motor skills or reduced fine motor skills
- Apraxia, difficulty with daily activities
- Seizures
- Spasms or spasticity
- Paralysis or muscle weakness
- Fatigue, inability to perform physical activities
- Sleep problems
- Decreased sense of smell or taste
- Hearing loss
- Vision loss, cerebral visual disturbances, eye problems
- Swallowing problems
- Urinary incontinence
- Constipation, slow bowel movements
- Pneumonia due to insufficient coughing up
advertisements are not ours
Resources
Neonatal subgaleal hematoma causing brain compression: Report of two cases and review of the literature
Arun P. Amar, Henry E. Aryan, Hal S. Meltzer, Michael L. Levy, Leslie N. Sutton, James M. Drake, Hajime Arai,
Alan R. Cohen
https://www.healio.com/ophthalmology/journals/jpos/1978-5-15-3/%7B84b4c1d3-0829-4c3e-911d-cda632cdf5d0%7D/posttraumatic-subgaleal-hematoma-extending-into-the-orbit-as-a-cause-of-permanent-blindness
Posttraumatic Subgaleal Hematoma Extending into the Orbit as a Cause of Permanent Blindness
J Reimer Wolter, MD; Gilbert J Vanderveen, MD; Richard L Wacksman, MD
https://www.ncbi.nlm.nih.gov/pubmed/15745253
Journal of Pediatric Ophthalmology and Strabismus. 1978;15(3):151-153
https://doi.org/10.3928/0191-3913-19780501-07
Cerebral palsy: causes, pathways, and the role of genetic variants,
https://doi.org/10.1016/j.ajog.2015.05.034
https://www.birthinjuryguide.org/brain-damage/
https://www.ncbi.nlm.nih.gov/medgen/589168
Evaluating the incidence and likelihood ratios for chromosomal abnormalities in fetuses with common central nervous system malformations.
Goetzinger KR, Stamilio DM, Dicke JM, Macones GA, Odibo AO
Am J Obstet Gynecol 2008 Sep;199(3):285.e1-6. doi: 10.1016/j.ajog.2008.06.100.PMID:18771985
https://www.kinderneurologie.eu/ziektebeelden/aangeboren/anencefalie.php
http://ghr.nlm.nih.gov/gene/FOXC1
https://www.kinderneuropsychologie.org/book/export/html/393
American Academy of Pediatrics, American College ofObstetricians and Gynecologists. Relationship between perinatal factors andneurologicoutcome. In: Poland RL, Freeman RK, editors. Guidelines forperinatal care. 3rd ed. Elk Grove Village, Ill.: American Academy ofPediatrics,1992:221-4.
Raichle ME. The pathophysiology of brain ischemia. AnnNeurol 1983;13:2-10
Anne M. de Grauw e.a.: Ontwikkelingsproblemen bij vroeggeborenen (2022) NTVG 166 nr. 1 blz. 42-46.; ntvg.nl/D6222
The definition an classification of cerebral palsy
Hersenletsel-uitleg: https://www.hersenletsel-uitleg.nl/soorten-hersenletsel-hersenaandoeningen/vanaf-geboorte-of-kindertijd/aangeboren-hersenletsel