Traumatic brain injury
Table of Contents
- Introduction
- Causes
- Three Types of Traumatic Brain Injury
- "Mild" Traumatic Brain Injury
- Memory Gap / Post-Traumatic Amnesia (PTA)
- Circulatory Dysfunction
- Neuropsychological Examination
- Coup and Contracoup
- Chronic Traumatic Encephalopathy
- Left or Right Damage?
- When No Damage Is Shown on the MRI
- Random Violence
- Traumatic Brain Injury Standard of Care
Traumatic Brain Injury
Traumatic brain injury occurs from an external cause, such as a blow, an accident, or violence. When a kinetic force from outside the body damages brain tissue, this can occur with or without a head injury.
Blood and fluid accumulate and take up space, pushing against the brain and potentially damaging it.
Nervous tissue is soft and fragile, and even slight pressure
can damage brain cells.
Traumatic brain injury here refers to physical, neurological suffering. The brain has been affected by external damage.
In case the circumstances have been psychologically extremely traumatic a PTSD (post-traumatic stress disorder) should not be ruled out.
Traumatic brain injury can vary in severity, with a concussion being the most severe form. This involves tearing brain tissue and blood vessels. The word "concussion" is not comparable to a concussion in any other part of the body. Most people with a concussion experience lifelong consequences. Some people recover (almost) completely.
The injury may be local (focal) or diffusely distributed throughout the brain.
Causes
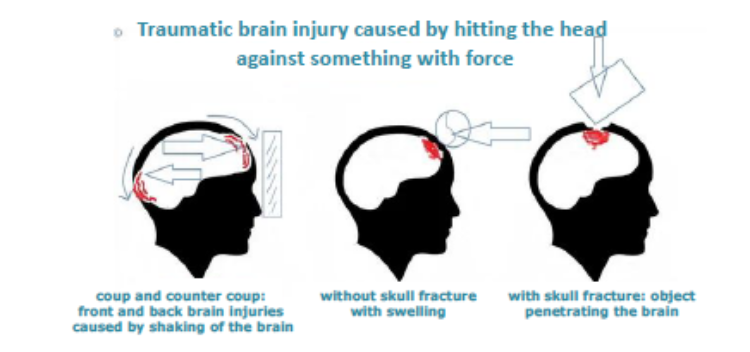
- Injury caused by an external force on the head, which may also damage the skull.
- Injury caused by one or more external objects penetrating the brain. In this case, there is always a skull injury.
Causes of traumatic brain injury due to force to the head may include:
- Being hit by another road user
- Being hit or kicked in the head
- Being hit by an object
- Falling headfirst onto the ground, for example, from a bicycle, horse, scaffolding, or stairs, and landing awkwardly
- Being near an explosion, for example, in a war zone
- Random violence
Possible causes of an injury involving an object penetrating the brain:
- A bone fragment that has penetrated the brain due to a skull fracture.
- An object such as a bullet, shrapnel, a stabbing weapon, or an iron object from an accident that has penetrated the brain. In such cases, the cause of the injury is not increased pressure on the brain, but the object that damaged it.
- In most cases, traumatic brain injuries are caused by sudden deceleration or acceleration of the head as shown in the image below.
Types of Traumatic Brain Injury
- A cerebral contusion occurs when a person has been unconscious for at least 15 minutes and/or has a PTA (post-traumatic amnesia or memory lapse) lasting longer than 60 minutes. This is the most serious form of traumatic brain injury.
- Residual symptoms after a concussion (post-concussion syndrome PCS or PPCS): a concussion may cause a brief period of unconsciousness. Sometimes there is no loss of consciousness! This is often referred to as a "mild brain injury," despite the often severe symptoms.
- Whiplash: in this case, the person has not been unconscious or for a very short time. Whiplash-Associated Disorder (WAD) is serious and often misdiagnosed. It is often referred to as a "mild brain injury," despite the often severe symptoms. Whiplash also has varying degrees of severity in terms of consequences. Whiplash often occurs simultaneously with a concussion.
Mild Traumatic Head Injury
Problems after Concussion and/or Whiplash
Most people recover from a concussion and/or or a whiplash, but it is less known and recognized that people may experience cognitive and/or physical problems after a concussion and/or a whiplash.
See our pages on Concussion (Commotio cerebri), Post-Concussion Syndrome (PCS) and whiplash
WAD.
These conditions are also called mild traumatic brain injury (mTBI). Although the name suggests that mild brain injury is a "light version," people with one of these conditions may experience significant symptoms.
The Memory Gap
Sometimes someone cannot remember anything about the accident or from the time before.
Usually, memories from just before the accident return quickly. It may also happen that someone cannot remember anything from the period after the injury. This is called post-traumatic amnesia (PTA). The lack of memory may persist for some time.
Because the brain doesn't store information during this time, PTA usually doesn't disappear afterward. Therefore, there's no point in continuing to search for these memories. In general, the more severe the traumatic brain injury, the longer the loss of consciousness and the memory gap, PTA, may last.
"The gap in memory (PTA)" is something completely different from filling the gaps in the failing memory with something else that seems most logical to the person. This is also called confabulating. It is not done consciously, and the person is not lying. He of she is convinced of the truth. See here for more information.
Circulatory Disorder
In case research methods have not detected brain damage and the patient continues to experience symptoms, it is not pretentious.
It was recently discovered that a circulatory disorder was detectable shortly after a concussion using a SPECT scan (contrast dye scan). A study in the US also found a circulatory disorder in 53% of people with long-term post-concussion syndrome (PCS).
Many people don't end up in this medical research mill after a concussion. A study comparing MRI and CT scans showed that the SPECT scan revealed more abnormalities in this area.
A biomarker (calpain-cleaved αII-spectrin N-terminal fragment (SNTF)) in blood predicts the risk of white matter abnormalities and cognitive complaints after mild traumatic brain injury. See the study about this here.
Neuropsychological evaluation
A neuropsychological examination may also reveal hidden cognitive damage, but it may be expensive.
In case a patient continues to experience significant symptoms and is diagnosed with a mild or mild brain injury, it is advisable to inquire about the possibility of this examanition, despite the costs.
This is especially true in case an MRI scan or a CT scan reveals nothing, the patient may be inclined to simply carry on, persevere, and keep pushing her- or himself.
Read more:
What happens in the brain during a traumatic brain injury?
The brain is the most complex and vulnerable part of the human body.
Its structure is similar to that of gelatin.
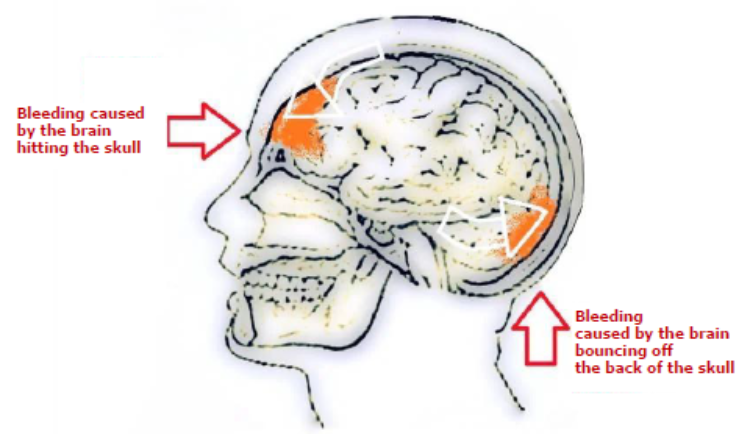
A blow, fall, or other impact shakes the brain back and forth, causing centrifugal force injuries to the back, front, or sides. See below:

Swelling and rupture of blood vessels occur on the side of the impact. This is called a coup. Because the brain moves more slowly than the skull, the brain first collides with the bone on the impacted side. Then the brain impacts the back or side of the skull. This is called a contrecoup.
A wikipedia page on coup contrecoup can be found here.
Bruising and rupture of blood vessels may also occur on the back or side.
This results in damage to both the front and back. At a microscopic level, not visible on MRI, the brain cell bodies are torn away from the axons of those brain cells, which transmit all signals to other brain cell bodies.
After this tearing, both the axons and the brain cell bodies die within seconds. These dead brain cells can no longer communicate with the others.
During the death, chemicals are released, and the neurotransmitters cause further damage because they are toxic to brain tissue.
The injury then spreads to the immediate vicinity of the affected brain cells. This damage continues for up to 24 hours after the initial impact. That's why medical intervention in the first 24 hours after an accident is so important.
Below some are videos about the death of axons and brain cell bodies in traumatic brain injury. The video on the left is only available on YouTube.
https://www.youtube.com/watch?v=55u5Ivx31og
Chronic Traumatic Encephalopathy
Experiencing multiple concussions may also cause brain damage.
Think of boxers who are frequently hit or soccer players who are hit hard on the head.
Research shows that they have a high risk of brain tissue deterioration.
See our page on Chronic Traumatic Encephalopathy (CTE).
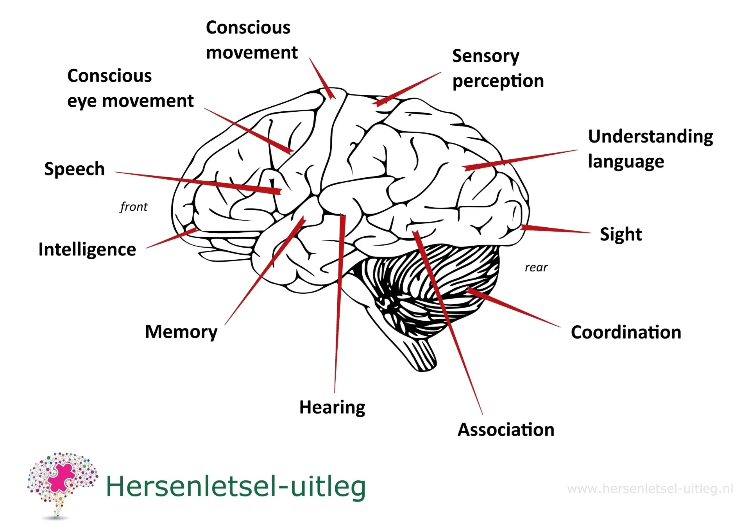
Left-sided damage or right-sided damage?
Generally speaking, the left side of the brain controls the right side of the body. For most people, language functions are located on the left side. The right side controls the left side of the body.
Damage to the right hemisphere leads to increased impulsivity, irritability and problems with spatial awareness. Read about damage to the left hemisphere. Read more
Functional areas may fail completely or become less effective.
However, the entire brain works together, and a function is driven by multiple structures.
Physical, cognitive, and/or behavioral consequences
Besides physical consequences, cognitive disorders may also occur. These relate to cognition: thinking, language, memory, concentration, the ability to absorb and process knowledge, perception, awareness, and attention. Cognition is a broad concept.
We list cognitive consequences on this page.
Behavioral consequences may also occur. This most commonly occurs with damage to the front of the brain, in the frontal lobe. Damage in this area may potentially result in frontal syndrome.
The frontal lobe is responsible for, among other things, controlling behavior and critical, judgmental thinking.
If this is disrupted, the person may exhibit disinhibited, apathetic, or egocentric behavior. It is also possible for someone to exhibit antisocial or rude behavior.
Skull Base Fracture
A skull base fracture is a break in the base of the skull.
This type of fracture usually occurs due to a severe impact to the head, such as a traffic accident, a fall from a significant height, or a sports injury.
Symptoms may vary, but common signs include bleeding from the nose or ears, bruising around the eyes (also called a "spectacle hematoma"), and in some cases, cerebrospinal fluid leakage.
A basilar skull fracture often accompanies a traumatic brain injury. Infections may also occur.
Skull Fracture
A skull fracture is a break in the skull, often caused by a hard blow to the head, such as a fall, traffic accident, or sports injury. Depending on the severity, a skull fracture can be accompanied by symptoms such as headache, nausea, dizziness, loss of consciousness, or neurological complaints, but the risk is particularly high for traumatic brain injury.
There is also a risk of an epidural hematoma.
In case no abnormalities are seen on the MRI scan
People with brain injuries that are invisible sometimes lead limited lives and are overdemanded and overestimated by those around them because nothing is visible.
Even an MRI scan often reveals no damage, but the injury can have significant life consequences because brain connections have been lost.
Read more about diffuse brain injury.
Read our page "When You're Not Believed" and the page with explanations
about what can and cannot be seen on each scan.
Random violence
In the Netherlands, the risk of brain injury resulting from violence is highest among young people aged 15 to 24.
Figures from VeiligheidNL from 2007 to 2011 show that an average of 2,200 victims of violence with brain injury visit the Emergency Department each year.
Traumatic Brain Injury Care Standard
In the Netherlands, work is being done on a care standard for traumatic brain injury.
See the page about this on the website of the Hersenstichting.

We list some websites in the US and in England about aftercare for (traumatic) brain injury:
https://www.facs.org/media/vgfgjpfk/best-practices-guidelines-traumatic-brain-injury.pdf
https://pmc.ncbi.nlm.nih.gov/articles/PMC5809702/
https://www.nice.org.uk/guidance/ng232
https://www.ninds.nih.gov/health-information/disorders/traumatic-brain-injury-tbi
https://biausa.org/brain-injury/about-brain-injury/treatment/brain-injury-rehabilitation
https://www.headway.org.uk/media/3320/bsrm-rehabilitation-following-acquired-brain-injury.pdf
advertising is not from our website
Resources
hersenletsel-uitleg.nl: https://www.braininjury-explanation.com/types-of-brain-injury-brain-disorders/traumatic-brain-injury
neurological aspects of long term outcome prognosis in paediatric closed head injuries Ruijs,hersenkneuzing.nl, Omgaan met hersenletsel Palm, frontiers in neuroloy, neurotrauma, gezondheidsraad hersenletsel bij boksers en voetballers, Left brain rightbrain Springer & Deutsch, Rowland, L. P. 2000, ‘Trauma - head injury’, in Merritt's Textbook of Neurology, ed L. P. Rowland, 10th edn, Williams and Wilkins,Baltimore.J.B.M. Kuks, J.W. Snoek, H.J.G.H. Oosterhuis. Klinische Neurologie 15e druk, Bohn Stafleu Van Loghum, Houten, 2003
Zomeren, A.H. van, & Burg, W.H. van den (1985). Residual complaints of patiënts two years after severe head injury. Journal of Neurology, Neurosurgery and Psychiatry, 48,21-28