Cognitive consequences
Explanation of cognition and the cognitive consequences of brain injury
The word "cognition" refers to everything related to thinking. It refers to how your brain works to perceive, understand, remember, and use that knowledge.
When you have a brain injury these functions may be affected. This is called cognitive impact.
Cognitive impact can be visualized using a Neuropsychological Examination.
Alphabetical order cognitive consequences
- Attention and concentration
- Apathy, showing little to no initiative
- Anosognosia (reduced or no insight into illness or one's limitations)
- Brainfog
- Cognitive pyramid
- Cognitive overstimulation
- Communication difficulties
- Decreased awareness
- Delayed information processing
- Delirium
- Difficulty with arithmetic and numbers or with figures, quantities, or the sequence of digits (dyscalculia)
- Disharmonic intelligence profile
- Executive functions
- Giftedness and brain injury
- Inability to do two things simultaneously
- Inability to recognize facial expressions
- Knowing that and knowing how
- Lack of overview and structure
- Memory
- Memory problems
- Navigation difficulties
- Neglect
- Orientation problems in person, place, time, and space
- Perseveration; Stuck and continuing with the same thing
- Problems with planning and organizing due to a lack of overview and structure
- Reduced flexibility
- Reduced stress resistance
- Reduced or no insight into illness
- Social cognition
- Start-up difficulties
- Time perception disorder
- Verbosity / constant talking, excessive talking
- Visuospatial and visuoconstructive problems, two problems with important cognitive functions for complex visual-spatial tasks and planning
- Visuospatial neglect, not perceiving what is happening on the affected side and in space
Cognition may affect:
- Emotions, Behavior, Relationships
- Language problems (pragmatic language disorder, taking language literally, word-finding problems)
- Problems with recognizing things, perceiving (agnosia)
Note! Cognition may be affected by other disrupted processes in the body.
Consider, for example, heart failure (decompensatio cordis).
In this case the brain receives less blood due to the failing heart.
In addition to physical symptoms symptoms may include drowsiness and confusion.
Cognitive problems occur in the areas of knowledge, understanding, perception, and comprehension. Difficulties with memory, concentration, and thinking speed are the most common.
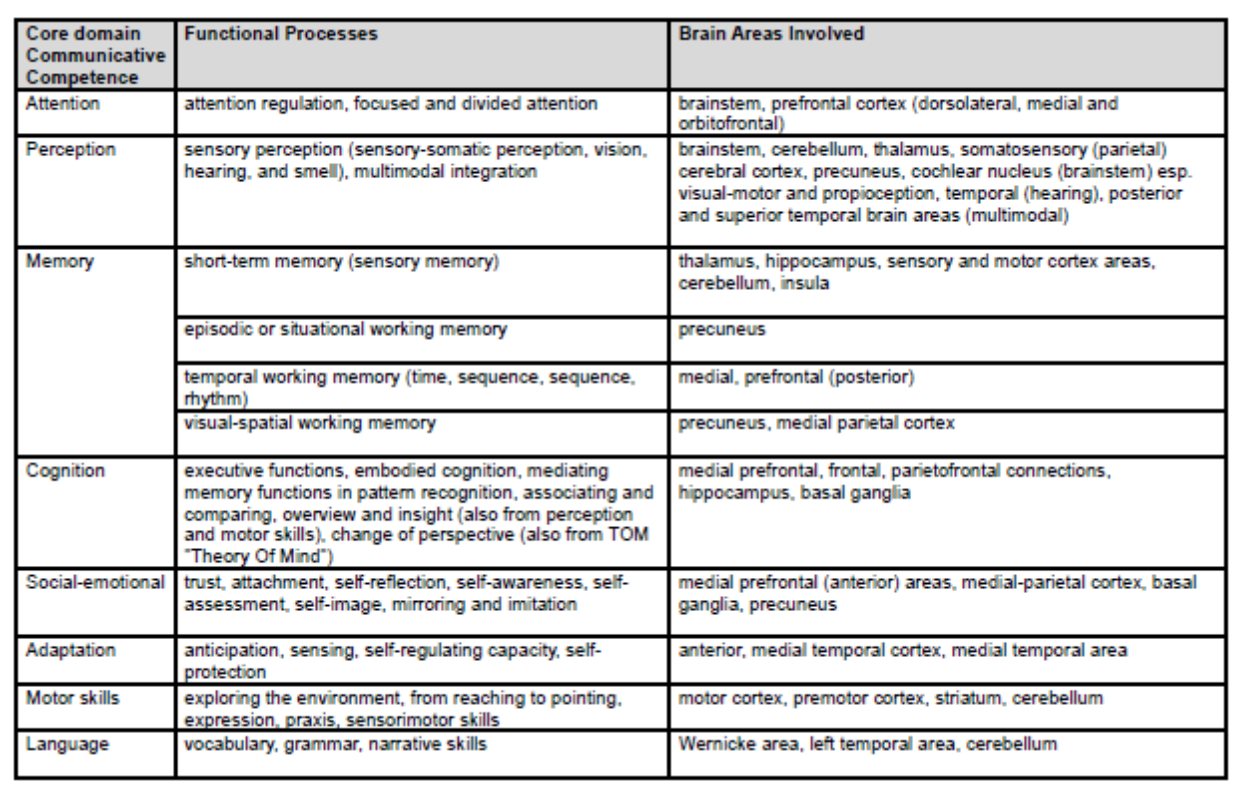
- Basic cognition includes: attention, learning, memory, perception, thinking and language.
- Metacognition includes: judgment, reasoning and a sense of reality.
- Social cognition includes: emotion, practical language skills and empathy.
Brain injury may have a significant impact on various aspects of daily life, including intelligence. However, intelligence is a complex concept that depends not only on one specific brain area, but on the collaboration of multiple areas within the brain.
Every brain injury is unique. Some people retain all of their intelligence, while others experience challenges in certain areas but maintain their intelligence in others. They may also experience difficulty with certain cognitive functions, such as information processing speed, memory, problem-solving, or concentration, while retaining all knowledge.
If someone struggles in certain areas, we call this a disharmonious intelligence profile.
See the dedicated page on that topic.
With a brain injury, it's both an advantage and a challenge that intelligence and analytical skills remain intact.
It offers relief: "The head still works."
A damaged brain often has to work twice as hard to compensate for residual symptoms. Think of a lack of cognitive flexibility, reduced concentration, and difficulty planning. This constant compensating is exhausting for the person involved and isn't always successful.
There are times when a coping strategy isn't sufficient, and then things go wrong.
Both the person affected and those around them often overestimate a person's capacity, leading to disappointment and misunderstandings.
Special challenges for people with brain injury and high intelligence
Six insights to remember
- Giftedness is more than just intelligence. It's about how someone thinks, feels, and processes things.
- Brain injuries affect gifted individuals differently. They lose not only their functions but also their cognitive abilities.
- Camouflage is a pitfall. These people score average or well on tests, but function far below their own standards. As a result, recognition is missed.
-
Standard care often doesn't suffice. Customized care, in-depth support, and recognition are essential.
- Support begins with recognition. This means acknowledging the gifted profile and the grief over the loss.
-
Group therapy often doesn't work. The group emphasizes adaptive behavior at the expense of individual therapy.
The combination of brain injury and giftedness can be particularly challenging. Gifted individuals often possess faster, more creative thinking and strong analytical skills, along with an IQ above 130.
Many gifted individuals not only think faster and remember more, but also have a different way of learning and approaching problems.
Gifted individuals are quick to analyze and see connections.
They value independence and autonomy, have intense interests, and a strong sense of justice.
When a brain injury occurs, these qualities can be compromised.
This may lead to frustration, confusion, and a sense of loss of self-identity.
The urge to learn may still be present, even strong, but is sometimes hampered by, for example, memory problems. This can be extremely frustrating.
Gifted people are often more aware of their limitations after a brain injury, which can increase the emotional impact. Furthermore, the complex effects of a brain injury can cause intellectual abilities such as concentration, memory, planning, maintaining an overview, and problem-solving to no longer function at their previous level.
Read more on the "disharmonic profile" page. The identity of a quick thinker may sometimes be completely lost, which can cause immense grief.
Gifted individuals often develop compensatory strategies to circumvent or compensate for cognitive limitations with their minds.
While this is incredibly helpful, it requires a tremendous amount of energy, which is often already limited. Neurofatigue is debilitating.
A person may be on the toes for a long time, trying to keep everything in check, until he or she reaches a complete standstill because all reserves have been depleted. A brain injury burnout is looming.
This can actually prolong the recovery time after a brain injury.
It's also unfortunately common for those around you to doubt the existence of a brain injury because "the head is still so strong". There seems to be a persistent misconception that having a brain injury automatically means someone has lost her or his intelligence.
This distrust from those around you can make you feel alone in your search for who you are with a brain injury.
Group therapy is often not effective. The group dynamic may lead to altered behavior, which can be disadvantageous to individual therapeutic progress.
Brain injury always impacts daily functioning, but for gifted adults, it can be even more complex and severe. Standard care often doesn't connect well, leading to an increased risk of misunderstanding and underdiagnosis.
Those who are both highly intelligent and highly sensitive face a dual challenge.
Brain injury may lead to physical, cognitive, and emotional limitations, such as fatigue, difficulty concentrating, and difficulty processing stimuli.
For highly sensitive people, who are naturally more sensitive to stimuli like sound, light, and the emotions of others, this may have a dual effect.
Sensing other people's emotions, such as the grief of a partner and children over the changed situation caused by a brain injury, may lead to a person pushing his or her own emotions and processing the brain injury into the background.
This requires extra attention to self-care, clear communication, and a low-stimulus, supportive environment.
There is a clear need for a personalized and careful approach, where we look not only at the symptoms of brain injury, but also at the unique needs and talents that come with giftedness.
How to cope with it: tips for professionals and stakeholders
- Be alert to giftedness: If you suspect it, seek specialized help.
- Recognize giftedness: Use this as a starting point for guidance and therapy.
- Work individually: Connect to the individual's level, offer substantive challenges, and take limitations into account (for example, by keeping sessions short, summarizing the conversation, and writing it down).
- Communicate transparently: Identify the tension between ambition and limitations.
- Balance between workload and challenge: Create tasks that provide just the right amount of stimulation without being overwhelming. This won't happen overnight, so keep exploring what works. Constantly evaluate how things went and learn from them. If necessary, document this in a schedule.
- Encourage meaningfulness: Actively seek new sources of meaning and fulfillment.
- Support the grieving process: Help with accepting loss without setting the bar too low. Recognition of the loss that the person experiences is essential, even though he or she can still do a lot.
- Encourage peer support: Contact with other gifted individuals with brain injury may support their recovery. Not everyone will need this, given the autonomous nature of many gifted individuals, but it's always worth trying.
The above tips are derived from the Dutch white paper that can be downloaded below.
What is a high EQ? How does brain injury affect it?
EQ stands for emotional intelligence: the ability to consciously manage your own feelings and those of others. How do you communicate? Can you show empathy, solve problems together, and build lasting relationships?
A brain injury can affect these skills. While empathy may not change internally, the need to maintain one's own boundaries can create an inner conflict in someone with a brain injury.
People with brain injuries and a damaged, underpowered inner battery pay the price when they try, at their own expense, to give others the same space they could once effortlessly offer. It has been proven that listening requires more effort for people with brain injuries than speaking.
However, some have changed in their empathy or in their ability to communicate effectively. We have written other pages about this.
Difficulty controlling impulses
People may find it harder to control their impulses. The brakes are off.
For example, someone might swear more quickly if something doesn't work out.
But someone might also eat and snack without inhibition.
People may be uninhibited when it comes to sex. Read about changed relationships, intimacy, and sexuality.
Injury to the frontal lobe, in particular, causes problems with impulse control. Teenagers with brain injuries where the frontal lobe hasn't yet fully developed can also have difficulty with this.
Lack of initiative/apathy
After a brain injury, a person may lack initiative. They may experience decreased activity and a lack of engagement. They may appear listless, indifferent, lack emotional expression (emotionally flat), and be difficult to motivate. There appears to be no correlation between the severity of the injury and apathy, nor between the duration of the brain injury and apathy.
Apathy is described as "a persistent decrease in motivation, responsiveness, and goal-directed behavior. It meets specific diagnostic criteria that distinguish it from depression."
The word apathy comes from the Greek word apatheia (ἀπάθεια). A = without or none. Pathos = suffering or passion.
Apathy is a syndrome of primary loss of motivation that cannot be attributed to impaired consciousness, cognitive impairment, or emotional problems.
Apathy can manifest as, among other things, a lack of goal-directed behavior, a decrease in goal-directed thinking, and emotional indifference with a flat affect (feeling). (Marin 1991)
In whom and how often does apathy occur?
Apathy is seen in neurological disorders such as Alzheimer's disease (63-90%), Frontotemporal dementia/FTD (92%), Vascular dementia/VD (72%), Lewy body dementia (57%), Progressive Supranuclear Palsy/PSP, CADASIL, Parkinson's disease, and Huntington's disease.
It also occurs in brain injuries such as stroke (36%), traumatic brain injury (20-70% with an average of 49%), brain infections, and brain tumors.
Furthermore, apathy occurs in several mental health conditions (including depression, PTSD, and schizophrenia).
Furthermore, apathy is a warning sign of dehydration, exhaustion, liver failure, poisoning and substance use (e.g., cannabis or alcohol), shock, underactive thyroid (hypothyroidism), and other conditions.
Rule out illness, depression, and medication side effects
Apathy can be a direct consequence of the brain damage itself.
Sometimes apathy is a symptom of another condition or of depression, as mentioned in the paragraph above. Therefore, it is important to rule out illness or possible depression. If depression is diagnosed, the depression should be treated first. It is also important to distinguish apathy as a side effect of medication. Discuss this with your doctor.
Recognize, acknowledge, and treat where possible
Apathy after a brain injury can be a barrier to rehabilitation and recovery. Therefore, it is important to recognize, acknowledge, and treat apathy where possible.
Where in the brain?
Apathy has been linked to damage to several brain areas, including the frontal lobe, basal ganglia, and cingulate gyrus. A blockage of dopamine pathways also appears to play a role.
How to approach?
It is important to approach a person exhibiting apathetic behavior with clear and repeated "gentle encouragement." Establishing a consistent structure and automatisms is recommended. The goal is for the person to perform as many routine tasks as possible, such as bathing, dressing, and other personal care tasks (if possible), independently.
Certain medications may have beneficial effects in reducing apathy. However, their effectiveness is not always clearly proven. Setting very specific goals can also help.
Continue to offer sufficient water, tea, or other drinks to prevent the person from becoming apathetic due to a lack of fluids.
Caregivers
It is often difficult for those around them when someone completely loses initiative and seems disinterested in anything. That's why it's important for the partner or caregiver to monitor their own load tolerance and health and to seek support if needed. See, for example, the CaregiverStrain Index on this page.
Limited flexibility
After a stroke or traumatic brain injury, people often struggle to cope with change or adapt to new situations. If something doesn't go as expected they may become completely disoriented.
This can lead to difficulty switching between tasks or finding solutions to unexpected problems. This is often because the brain processes and coordinates signals less effectively after an injury.
Unexpected visitors or a setback, for example, are difficult situations.
People with brain injury experience difficulties switching from one task to another.
This also applies to switching from one thinking task to another, such as working on a computer and then switching to an unexpected phone call.
The brain itself is no longer flexible enough to handle such a switch to a completely different task.
If the conversation partner switches to a different topic this may also cause difficulty for the person with a brain injury.
This is not a matter of unwillingness, but of inability.
Stress tolerance may also decrease. During times of acute stress or major problems, all areas of the brain are activated simultaneously, creating a kind of short circuit.
Read our dedicated page on reduced stress tolerance.
Quotes from people who have become less flexible
- Sometimes, after a conversation ends, I have to come back to something because I can't interpret in time what I heard. It took me a little longer to find the right word, and then the conversation continued because I was lost in thought, or I got distracted again, or something was said (by me or someone else) that wasn't right, and it takes me a while to realize it...
- I am simply not as flexible anymore. I also generally perform my tasks a bit more slowly than before.
- If I am busy with something and a phone call comes in, I can't switch gears. I can't even think at that moment. Apparently, when you have brain injury, you try to focus on a task with all your might, so much so that you lose track if it has to stop abruptly and unexpectedly.
- During a conversation, I often can't adjust because I'm so busy trying to stay focused that I don't even think to ask for a moment's pause or to repeat something. Having a conversation can be very difficult, and even if the problem is identified beforehand, it's not always taken into account.
- I live a structured life, get up at set times, and do my activities. Even on vacation, I try to maintain my morning routine. That way, it doesn't take as much energy to get back on track after the holiday.
- People often underestimate how difficult it can be to learn new "tasks" and adapt to a different work environment or situation. It takes time to establish new routines, and you often quickly forget exactly how to do something. This happens, for example, when you start at a new job or stay in a different house or vacation home. Even small (learned) tasks, such as a morning routine at home (making the bed, getting dressed), or how to start at work (turning on the computer, preparing folders), can suddenly become a challenge. Getting used to a new situation or environment again is always a difficult adjustment.
More dependent
Some people become increasingly dependent on their partner or other loved ones. They let them have conversations, make arrangements, and do physical tasks. Their partner gradually takes over more and more, so the dependency worsens.
Our advice is to try to continue arranging things together and in case that exceeds the capacity of te person with brain injury, assign smaller tasks.
Cognitive pyramid
Cognitive functions have a certain hierarchical relationship with each other.
The functioning of a particular lower cognitive function in the pyramid will influence the functioning of a higher function.
Someone who struggles with memory may experience this due to problems with attention and concentration, and not simply because memory is impaired.
The reverse is also possible. Impairments in executive functions may impair the functioning of other cognitive functions.
Executive functions represent the higher level of control over basic abilities, which involves whether and how someone uses their knowledge, skills, and intellectual talent (Fasotti & Spikman, 2001).
Someone who is tired or overstimulated is no longer able to function because sensory perception is the foundation.
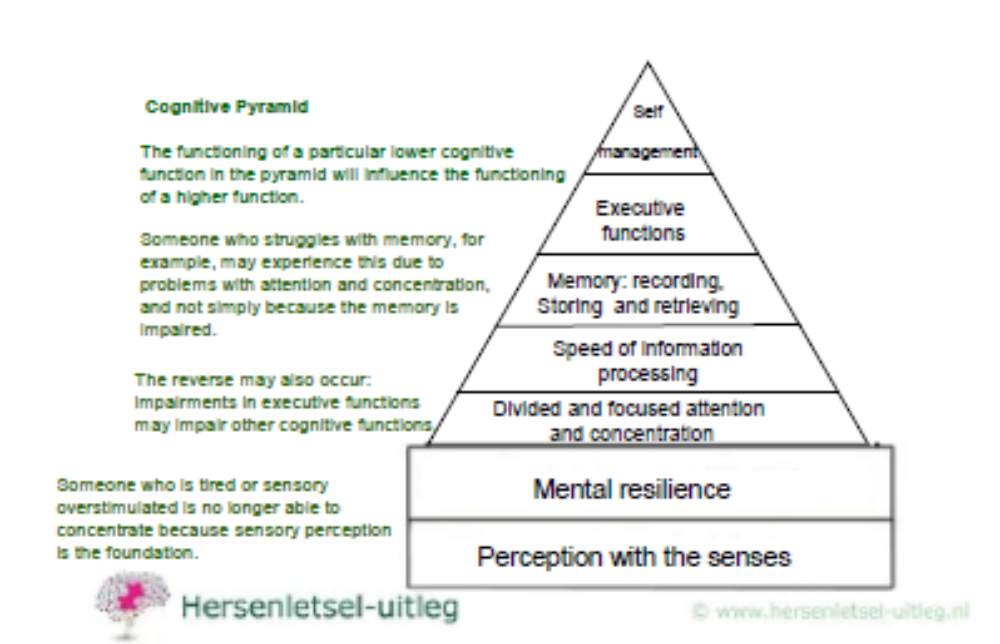
Pyramids are often used in literature to illustrate cognitive functioning. Several exist worldwide, each with a slightly different structure.
Our general pyramid model for overstimulation in brain injury is based on a framework that encompasses the neural networks of the autonomic nervous system and sensory systems.
Mental capacity fluctuates daily, and so does functioning.
We emphasize that you perceive with your senses and during perception you may become overstimulated due to poor filtering. The other layers of the pyramid lie above perception.
In case the base isn't functioning properly, the functions above it will not function properly either.
(Copyright J.van Haastrecht en A.van Schaaijk, team Hersenletsel-uitleg 2018)
advertisements are not ours
Resources
Grondslagen van de neuropsychologie Luria, Aandachtsstoornissen. Een neuropsychologisch handboek Eling& Brouwer, Omgaan met hersenletsel Palm,hersenletsel-uitleg.nl, Attention, mental speed and executive control after closed head injury, Spikman hersenstichting.nl, Cognitive psychology Neisser, NewYork, M.T. Banich (2004). Cognitive Neuroscience and Neuropsychology. 2e editie. Houghton Mifflin Cie en J.B.M. Kuks, J.W. Snoek, H.J.G.H. Oosterhuis.Klinische Neurologie 15e druk, Bohn Stafleu Van Loghum, Houten, 2003, ISBN 90-313-4028-6
Caeiro L, Ferro JM, Costa J. Apathy secondary to stroke: a systemic review and meta-analysis. Cerebrovasc Dis. 2013;35:23-39.Carson, A. J., MacHale, S., Allen, K., Lawrie, S. M., Dennis, M., House, A., & Sharpe, M. (2000). Depression after stroke and lesion location: a systematic review.The Lancet, 356(9224), 122–126.Chase T. Apathy in neuropsychiatric disease: Diagnosis, pathophysiology and treatment. Neurotox Res 2011; 19: 266-278.
Ciurli P, Formisano R, Bivona U, Cantagallo A, Angelelli P. Neuropsychiatric disorders in persons with severe traumatic brain injury: Prevalence,phenomenology, and relationship with demographic, clinical, and functional features. J Head Trauma Rehabil. 2011;26:116-126.
Jorge RE, Starkstein SE, Robinson RG. Apathy following stroke. Can J Psychiatry. 2010;55(6):350-4.
Lane-Brown AT, Tate RL. Apathy after acquired brain impairment: a systematic review of non-pharmacological interventions. Neuropsychol.2009;19(4):481-516.
Mikami K, Jorge RE, Moser DJ, et al. Prevention of poststroke apathy using escitalopram or problem-solving therapy. Am J Geriatr Psychiatry.2013;21(9):855-62.Marin, R. S. (1991). Apathy: A Neuropsychiatric Syndrome. The Journal of Neuropsychiatry and Clinical Neurosciences, 3, 243-254.
R.S. Marin et al. Reliability and validity of the Apathy Evaluation Scale Psychiatry Res (1991)
Marin, R. S., Biedrzycki, R. C., & Firinciogullari, S. (1991). Apathy Evaluation Scale (AES, AES-C, AES-I, AES-S) [Database record]. APA PsycTests. https://doi.org/10.1037/t28570-000
A. T. Lane-Brown & R. L. Tate (2009) Apathy after acquired brain impairment: A systematic review of non-pharmacological interventions,Neuropsychological Rehabilitation, 19:4, 481-516, DOI: 10.1080/09602010902949207
https://www.sciencedirect.com/science/article/abs/pii/S1627483013000020
Worthington A, Wood RLL. Apathy following traumatic brain injury: a review. Neuropsychologia. (2018) 118:40–7.
Cranenburgh, B. van (2002). Het belang van inzicht in het geheugen voor de revalidatie. Neuropraxis, 4(1):162-163.