Capsula interna
The inner capsula
The capsula interna is an important nerve, fiber bundle between the two brain hemispheres and therefore an important connection to the cerebral cortex, the corpus callosum and the little brain (cerebellum). It is also an important link connecting the thalamus to the prefrontal cortex.
The capsula interna contains nerves which both send and receive signals. It is comparable to a multi-lane highway with numerous intersections.
The capsula interna belongs to the subcortical brain structures (below the cerebral cortex) just like the brainstem, thalamus, nucleus caudatus, globus pallidus and putamen (part of the basal nuclei / basal ganglia).
The capsula interna has a white appearance because of the myelin sheath that surrounds the axons. (Myelin is comparable to the insulation layer around electrical wiring.)
The capsula interna contains both connections for the movements (motor neural pathways) as well as for the senses, more specifically for seeing and hearing (sensory neural pathways).
The pyramidal system, a kind of movement highway between brain, spinal cord and muscles, is for a large part located in the capsula interna. It ensures the control of the skeletal muscles.
The capsula is divided into five areas
- "Anterior, crus anterius" The front limb,
- "Genu" which literally means knee; a bend in the fiber track, switching station to motor areas. It contains bands that control the muscles of face and neck,
- Posterior, crus posterius" the rear part. It contains bands of acoustic fibers to the temporal lobe (temporal lobe) and visual fibers to the occipital lobe (occipital lobe),
- "Retrolenticular", pars retrolentiformis. It is located behind the lenticular core / nucleus lentiformis, consisting of putamen and globus pallidus. It contains pathways from the thalamus to the visual cortex. It contains reversed orbits that run from the temporal and occipital lobe to the sponge. It contains sensory fibers from the thalamus and pathways to the cortex where the association takes place.
- "Sublenticular", pars sublentiformis. It is located beneath the lenticular core / nucleus lentiformis, consisting of putamen and globus pallidus. It contains both tracks from the thalamus to the auditory cortex where sound is processed and images to the visual cortex where vision is processed.
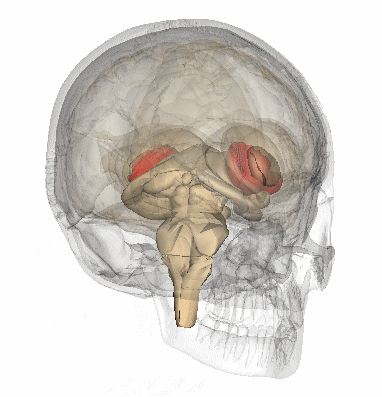
The image below on the left shows a cross-section of the brain. The top is the front of the brain where the eyes are located. The fiber web that forms the capsula interna is drawn in red.
The image below on the right is from: https://commons.wikimedia.org/wiki/File:Internal_capsule.gif

Small injury with extensive consequences
Injury in the capsula interna can give many different symptoms because both the nerves of the nerves can be affected as well as the sensory nerves and sensory nerves. Even a "small" stroke can have as great consequences as a major stroke in the cortex of the cerebrum or in the subcortical areas.
A stroke in the internal capsule inevitably leads to damage to the ascending and descending brain jobs.
Injury in the anterior part can lead to loss or weakness in the arms and face,
Injury in the genu can lead to damage in the frontal lobe and may result in a memory disorder,
Injury in the posterior part can result in an ataxia (walking disorder).
(Schmahmann, Rosene, & Pandya, 2004)
Possible complaints:
- Failure of arm, hand, leg, foot or face. The failure can manifest itself through half-sided weakness (hemiparesis) or paralysis (hemiplegia),
- Paralysis of the lower half the face,
- Reduced or incomplete sense perception in the arm, leg or face,
- Difficulty speaking clearly. Dysarthria,
- Word-finding problems without aphasia,
- Difficulty swallowing and chewing,
- Spasms, spasticity,
- Transient muscular contractions,
- Difficulty seeing in case of fatigue,
- Ataxic hemiparesis due to weakness, awkward gait, coordination disorder,
- Invisible consequences.
A stroke at the capsula interna can be ruled out as soon as someone has symptoms such as a glare or that the person has a stare or visual field failure, aphasia or neglect. These complaints only occur in case of injuries from the cerebral cortex.
The injury can be visualized with an MRI scan or CT scan, but if it is a minor infarct such as a lacunar infarct it can be difficult to visualize it on a scan despite the severe symptoms.
Most injuries in the capsula interna will not be fatal and some degree of recovery can be expected.
Possible characteristics of a stroke in the capsula interna
- Failure of face, arms or legs (pure motor stroke = PMS pure motor syndrome). This is the most common form of lacunar stroke. If an arm is affected as much as a leg, the injury is usually located in the capsula interna.
- Mixed failure of sensory and motor nerves; this gives weakness and loss of feeling on the other side of the body. In the medical terms this is called contralateral paresis and contralateral sensory injury.
- Dropping out of the upper motor neuron regions, causing the inhibitory effect on the muscles to fail. The doctor then sees the following symptoms:
- Sign of Babinski, the big toe goes up at a foot sole reflex test,
- Hyperreflexia, an increased response to stimuli (too high reflex),
- Clonus, transient muscle contraction,
- Spasticity, tense stiff muscles or muscle spasms. It shortens the muscles.
- Reflex by Hoffman, reflexive bending of the tip of the thumb tip and in particular the index finger tip, when the doctor squeezes the fingernail of the extended middle finger of the same hand.
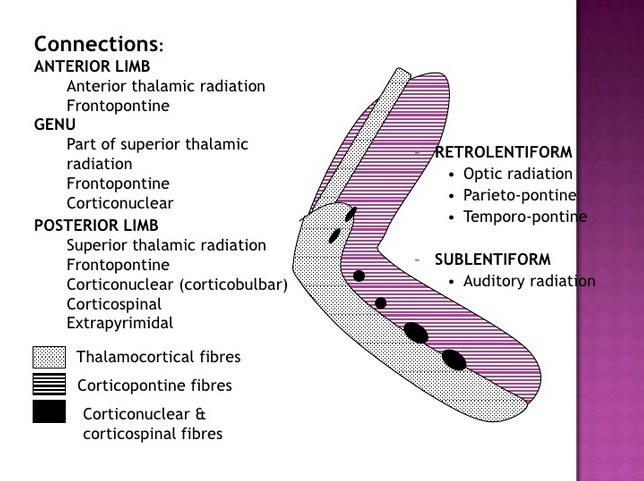
The image is from: https://www.slideshare.net/ananthatiger/internal-capsule
Thalamocortical fibers (gray in the image above) and, in reverse, the corticothalamic fibers are the pathways between the cerebral cortex and the thalamus.
Corticopontin fibers (purple in the image above) are the connections between the bridge (pons) and the cerebral cortex.
Extrapyramidal fibers in the posterior part.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4903141/
https://books.google.nl/books?id=1cPbFCXDyF0C&pg=PA377&lpg=PA377&dq=capsula+interna&source=bl&ots=O0wpbJzxzJ&sig=mRwV1HE4A9e71WsuFbYRyuo5d_s&hl=nl&sa=X&ved=2ahUKEwj0m7uvqcfeAhXKBSwKHRsLCrAQ6AEwDXoECAIQAQ#v=onepage&q=capsula%20interna&f=false
https://stanfordmedicine25.stanford.edu/the25/ics.html
https://radiopaedia.org/articles/internal-capsule
https://www.sciencedirect.com/topics/neuroscience/posterior-limb-of-internal-capsule